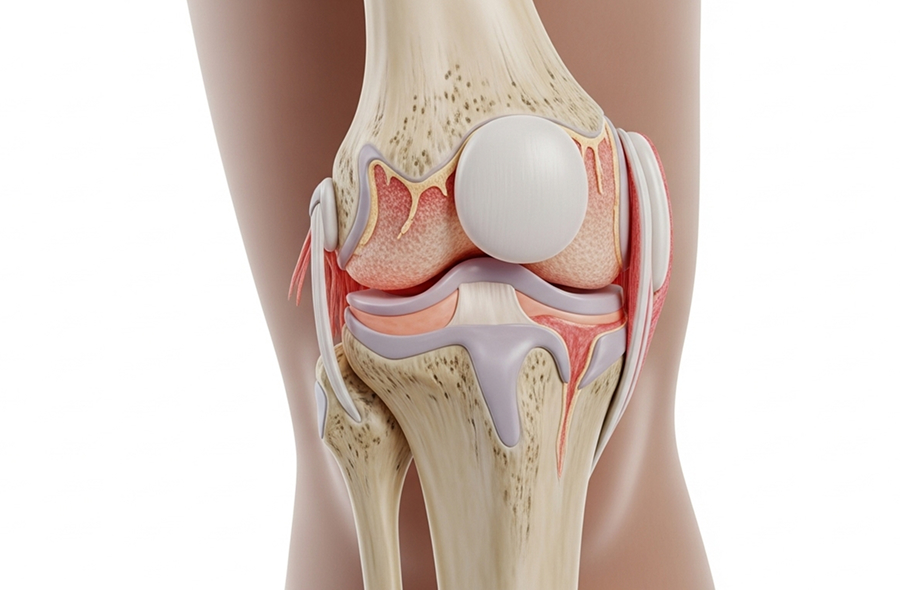
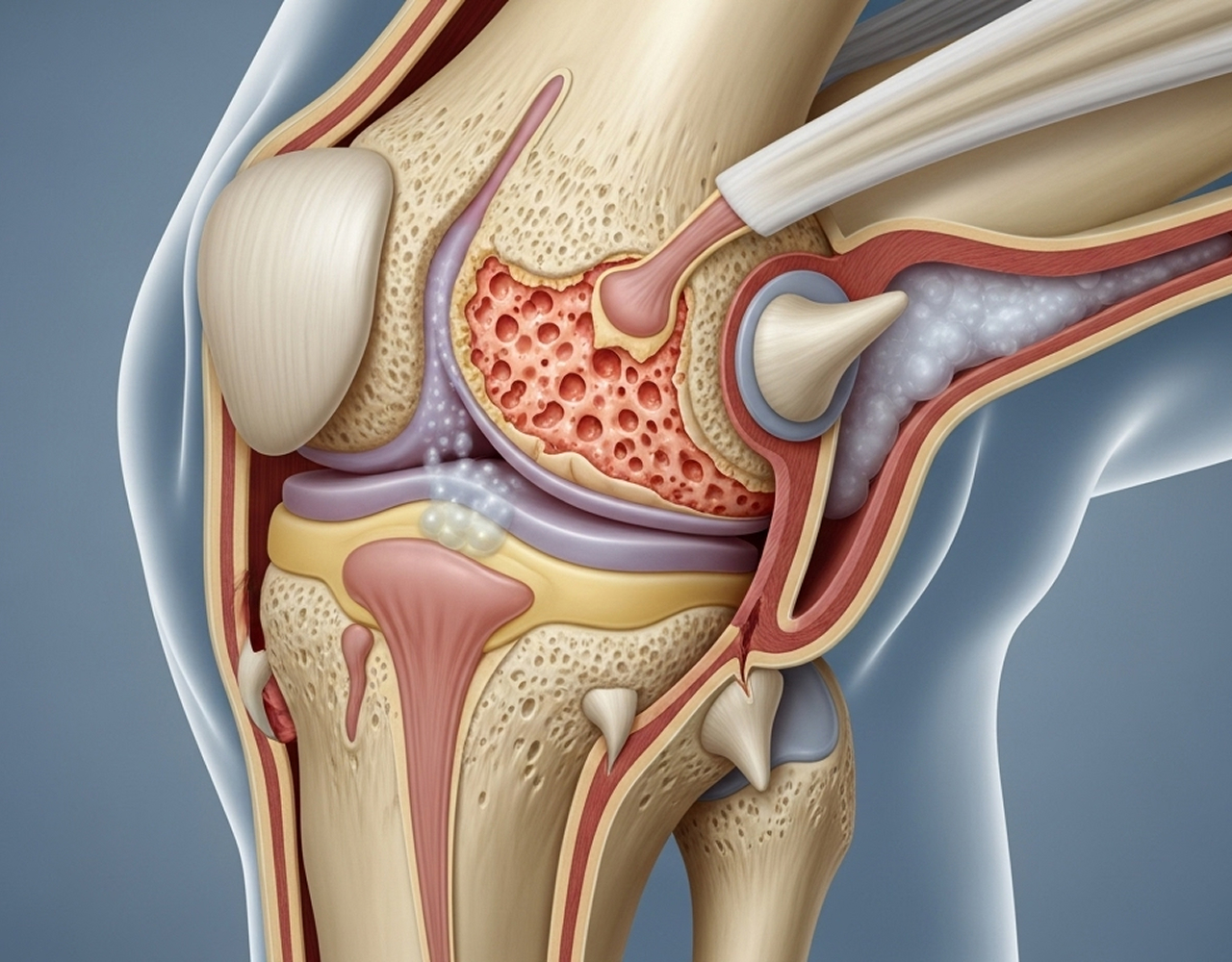
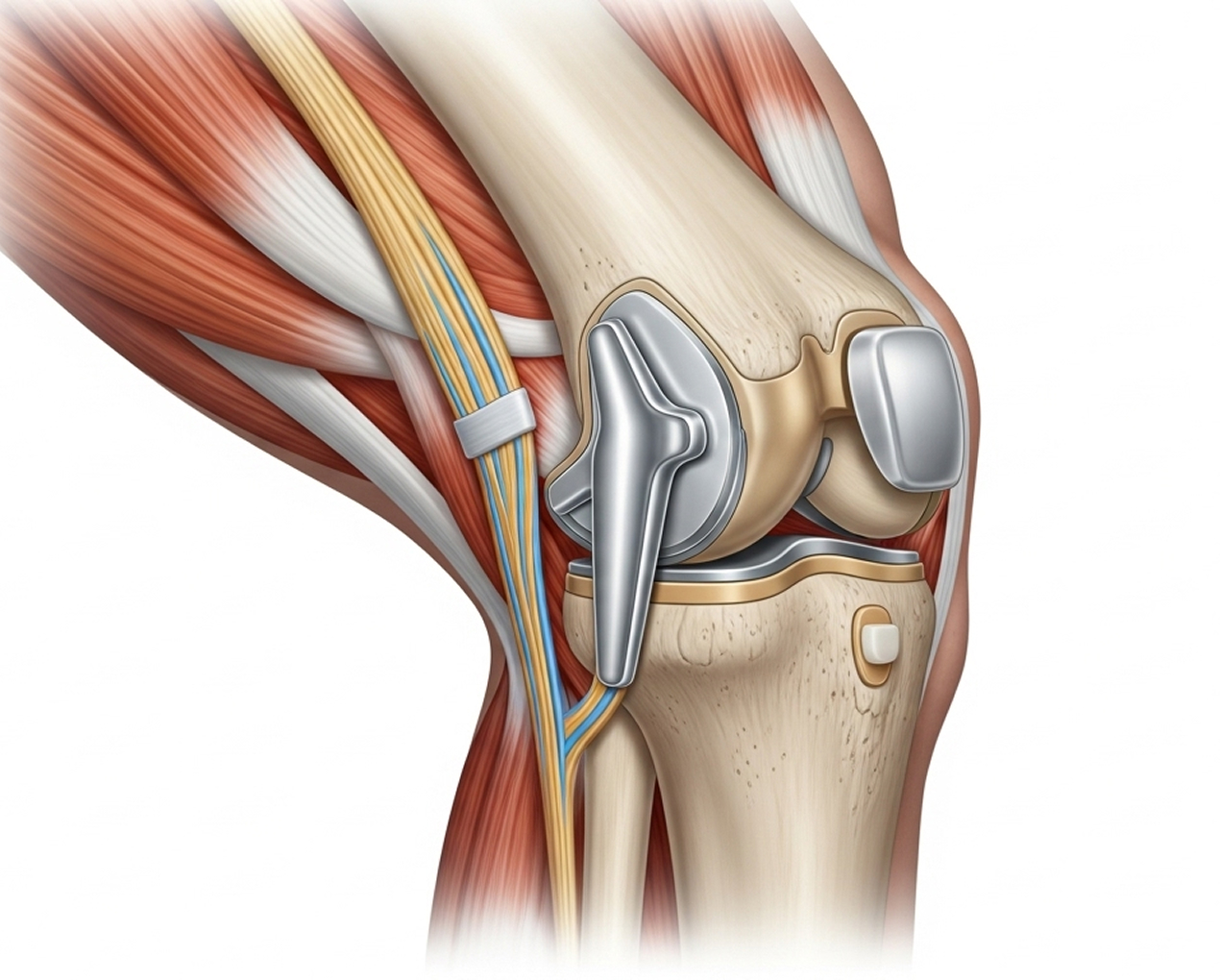
Total knee replacement (or total knee arthroplasty) is a highly successful surgical procedure to relieve the pain of severe knee arthritis. It involves resurfacing the damaged ends of the thigh and shin bones with prosthetic components, creating a new, smoothly functioning joint.
As a fellowship-trained knee subspecialist, Dr Richard Allom uses advanced techniques, including robotic-assistance and personalised alignment, to ensure the replacement fits your specific anatomy. The primary goal is to significantly reduce pain, restore movement, and improve your overall quality of life.




While personalised alignment shows excellent results, the primary considerations are the surgeon's experience and the technology required.
This approach demands specific subspecialist training and access to advanced robotic systems to execute the 3D-planned, patient-specific cuts accurately. This is an evolution of traditional techniques, and its successful implementation is highly dependent on the surgeon's expertise in the system.
Not every surgeon offers personalised alignment techniques. My subspecialist training and robotic surgery expertise enable me to provide this cutting-edge approach, potentially enhancing outcomes for my patients.

Modern knee replacement implants are designed to last 15 to 20 years or more. The Australian National Joint Replacement Registry reports 90-95% are functioning well at 10 years, and 85-90% at 15 years. Factors affecting longevity include your age at surgery (younger patients might eventually need revision), activity level, weight, surgical technique precision, and implant type.
Pain is managed using a multimodal approach (spinal anaesthesia, nerve blocks, oral medications). Most patients find post-operative discomfort manageable with prescribed pain relief. The first 2-3 days are typically the most uncomfortable, improving progressively. Long-term, 85-90% of patients experience significant pain relief compared to their pre-surgery arthritis pain.
Many patients can kneel after knee replacement, though it might feel different. Kneeling tolerance varies and improves with time and physiotherapy. It's not harmful to the implant to kneel. Any discomfort is usually related to soft tissue sensitivity around the kneecap, not implant damage.
Low-impact activities are generally encouraged: swimming, cycling, golf, doubles tennis, lawn bowls, hiking, dancing. Activities acceptable with caution include skiing (downhill), low-impact aerobics, and rowing. High-impact activities like running, contact sports, singles tennis, and high-impact aerobics are generally discouraged to preserve implant longevity. I provide personalised activity guidance based on your goals and circumstances.
Costs vary depending on your private health insurance coverage, hospital choice, and individual factors. As a private orthopaedic surgeon, I accept Medicare and private health insurance rebates. Gap fees apply. I provide transparent cost estimates during consultation, and my practice manager assists with insurance verification and financial planning.
If knee pain is significantly affecting your quality of life, a specialist assessment can determine if total knee replacement is the right option for you.
What to Bring: Please bring your referral letter, all relevant imaging studies (X-rays, CT scans, MRI if performed), and your list of current medications to your consultation.