Requires X-rays and a mandatory CT scan for precise three-dimensional surgical planning, often alongside an MRI to assess associated ligament or meniscus damage.
Surgical patients must commit to 6–12 weeks of strict non-weight-bearing, with full return to high-impact activities taking 9–12 months.

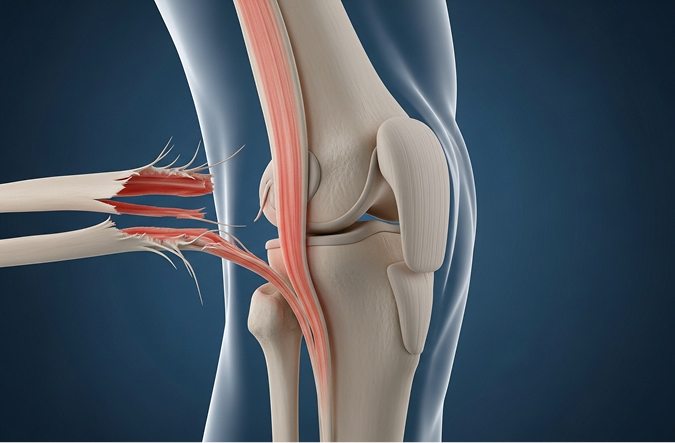
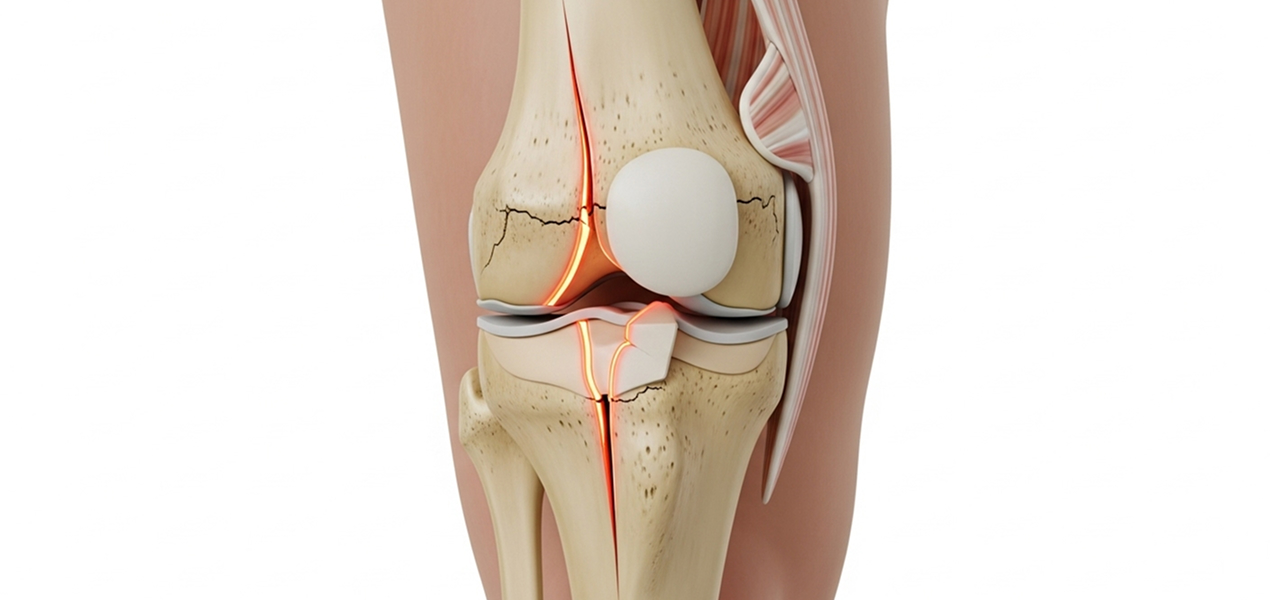
These injuries typically result from significant force applied to the knee, such as motor vehicle accidents, falls from height, or high-impact sports injuries. In older adults with weakened bones, fractures can occur from lower energy trauma.
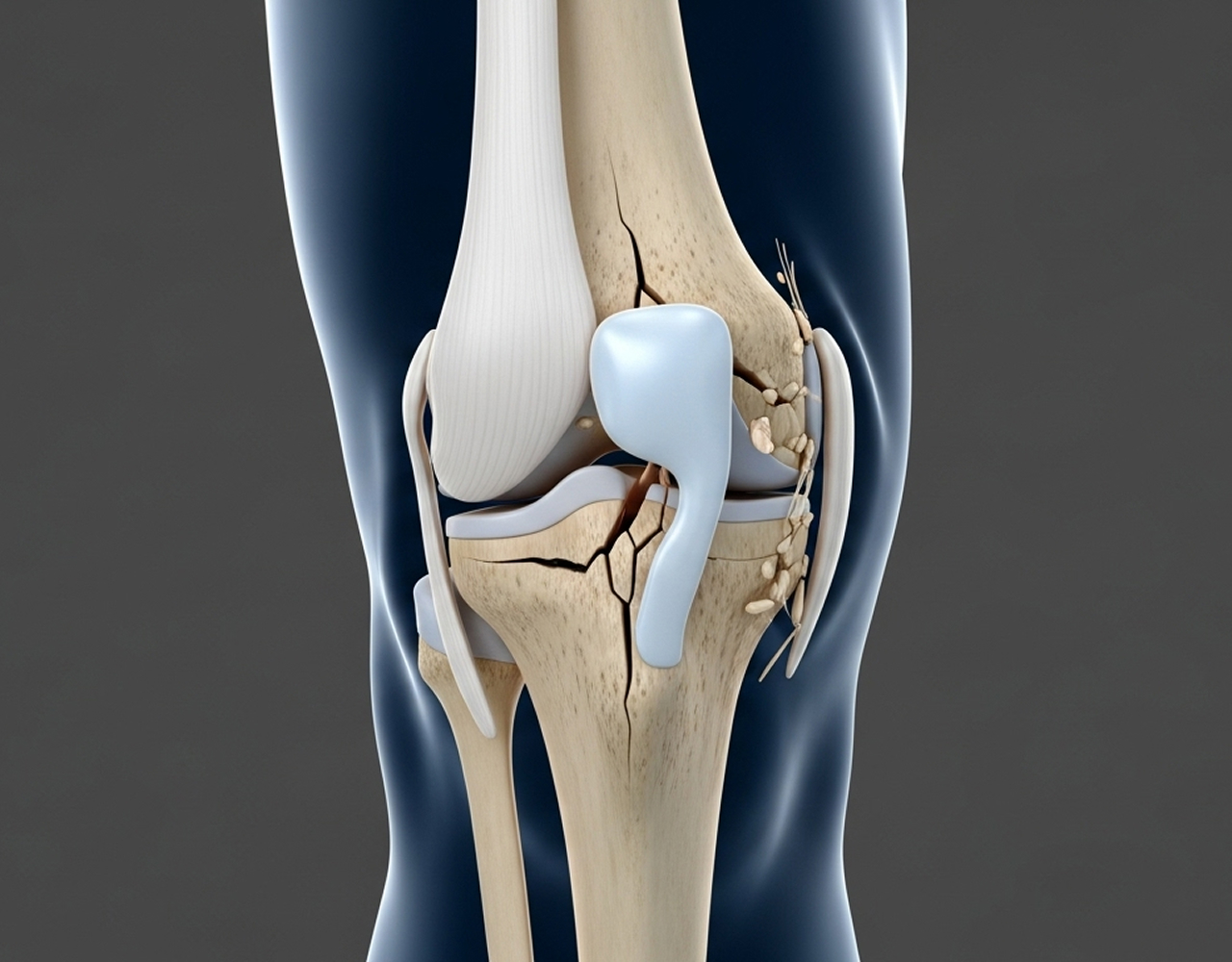
Orthopaedic surgeons classify these fractures using the Schatzker system (Types I–VI) to guide treatment:
Immediate symptoms include severe knee pain, rapid swelling, and the complete inability to bear weight on the affected leg. The knee may also feel unstable.
Accurate diagnosis and planning require comprehensive imaging:

Conservative care is reserved for minimally displaced or stable fracture patterns (typically less than 2–3mm displacement) with adequate bone quality. The protocol involves protection with a hinged knee brace and strict non-weight-bearing for 6–12 weeks, followed by controlled physiotherapy. Non-compliance risks fracture displacement, often necessitating surgery.
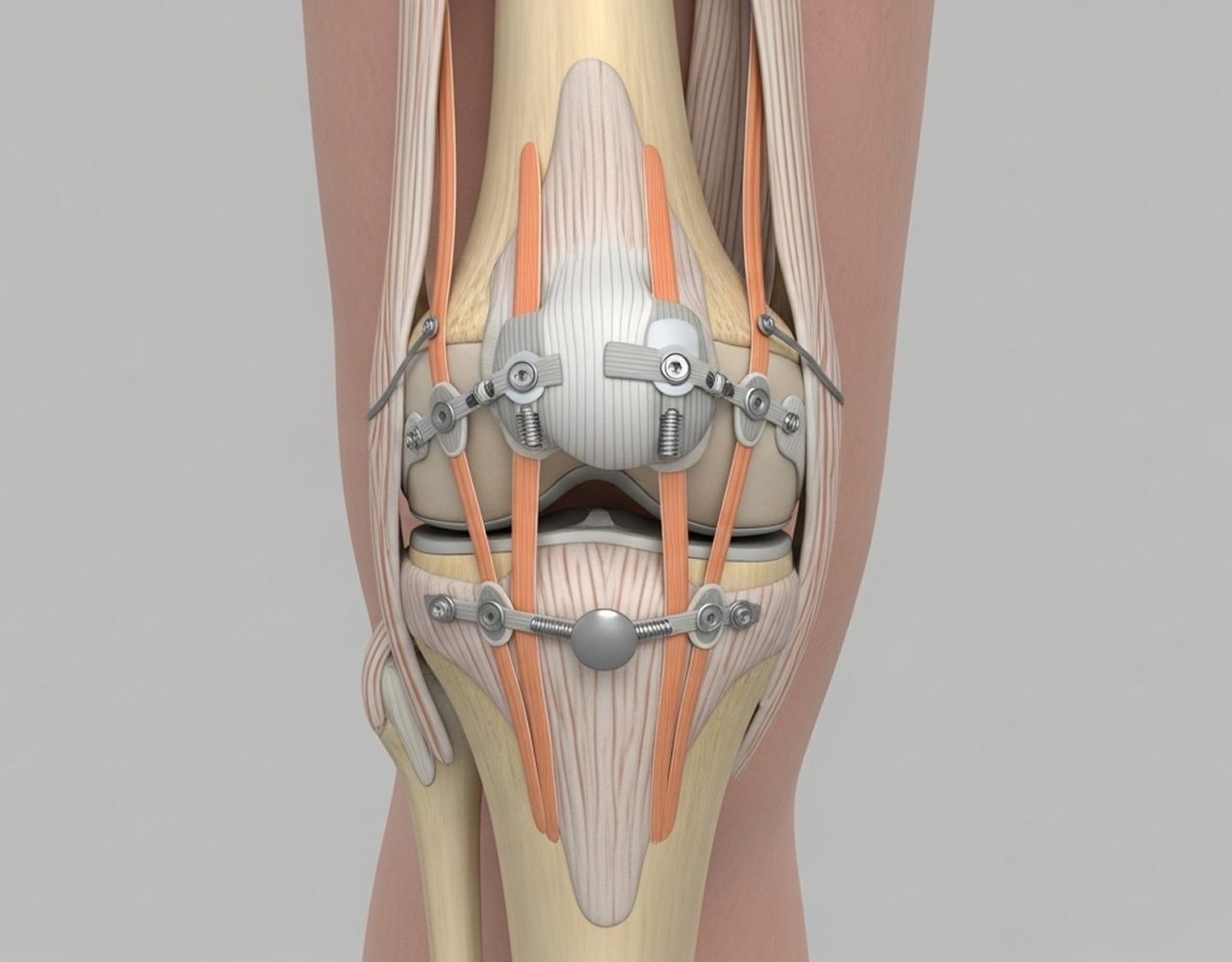
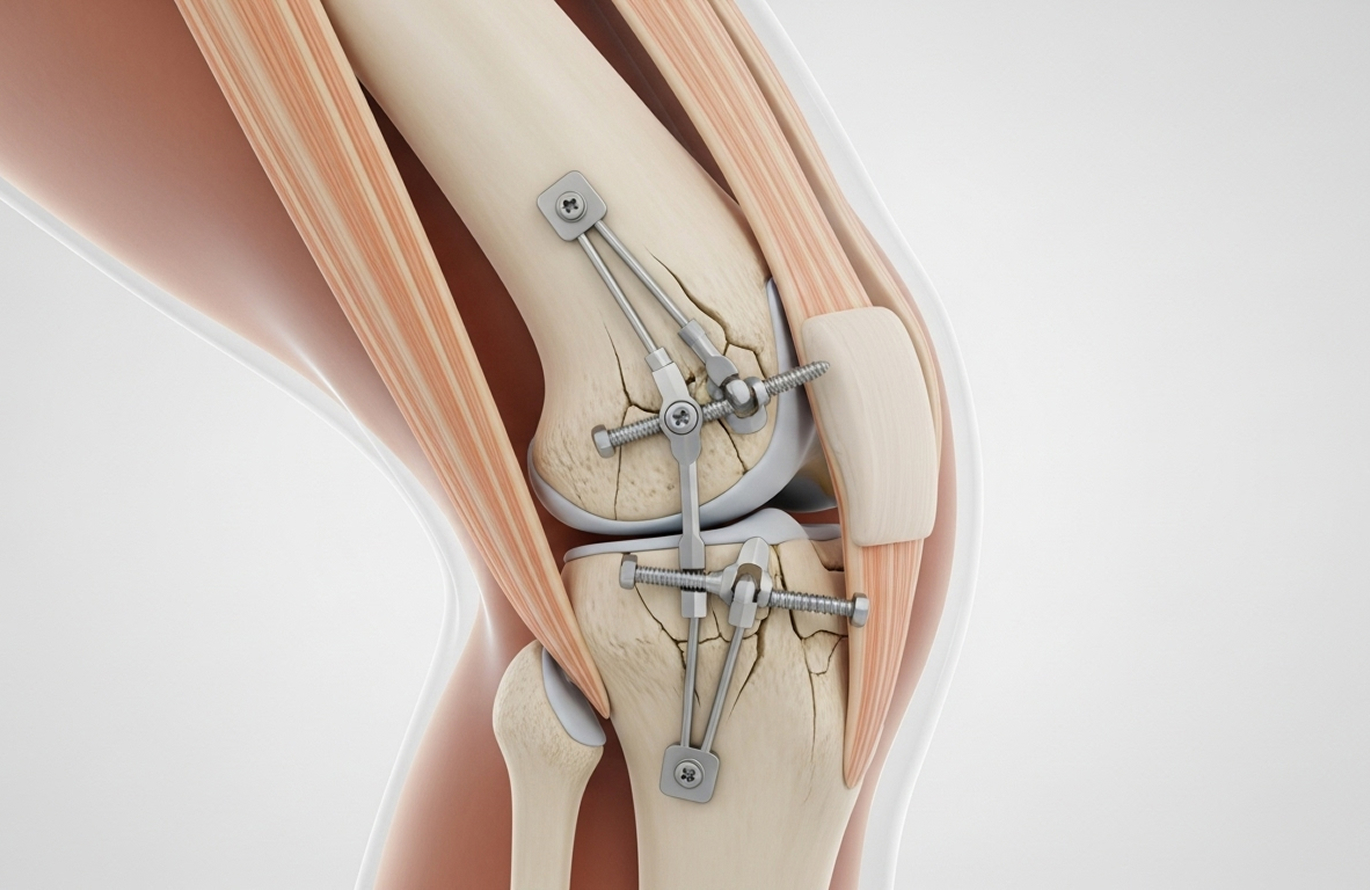
Most tibial plateau fractures require Open Reduction and Internal Fixation (ORIF) to restore the joint surface and mechanical alignment.
Depressed bone is elevated and the void is structurally supported using bone graft augmentation (autograft, allograft, or substitutes). Stable fixation is achieved with advanced locked plating systems and screws, allowing early range-of-motion exercises.
Strictly non-weight-bearing with crutches/frame. Gentle range of motion (passive). Managing swelling.
Important Note: Complex bicondylar fractures (Schatzker V–VI) typically require the longest recovery periods.
Complete functional recovery generally requires 3–6 months, but a return to high-impact sports takes a minimum of 9–12 months. Simple fractures heal faster (3–4 months for full activity), while complex bicondylar fractures require longer, up to 12 months.
Post-traumatic arthritis is a high risk. Research shows the incidence varies widely, but Dr Allom’s goal is to minimise this risk by achieving the most anatomic joint reduction possible. Regular follow-up allows for early detection and management.
Sedentary work usually resumes at 6–12 weeks. Light physical work at 3–4 months. Heavy manual labour requires 6–9 months. High-impact sports require 9–12 months minimum and medical clearance to prevent refracture or accelerated arthritis.
The metalwork (plates and screws) is typically left in place permanently if it is asymptomatic. Removal is necessary in about 10–20% of patients. We remove hardware if it causes irritation, pain under the skin, or develops a late infection. This removal procedure is usually a relatively straightforward day surgery performed once the fracture is completely healed.
Starting weight-bearing prematurely can have serious consequences. The fracture fragments may shift, causing the articular joint surface to collapse. This loss of alignment is called displacement. If this happens, it accelerates the risk of post-traumatic arthritis and often requires further surgery to re-stabilise the bone. Strict non-weight-bearing is essential to protect the surgical repair.
I welcome patients across South West Sydney and the Mid North Coast seeking expert management of complex knee fractures.
What to Bring: Please bring your referral letter, all relevant imaging studies (X-rays, CT scans, MRI if performed), and your list of current medications to your consultation.