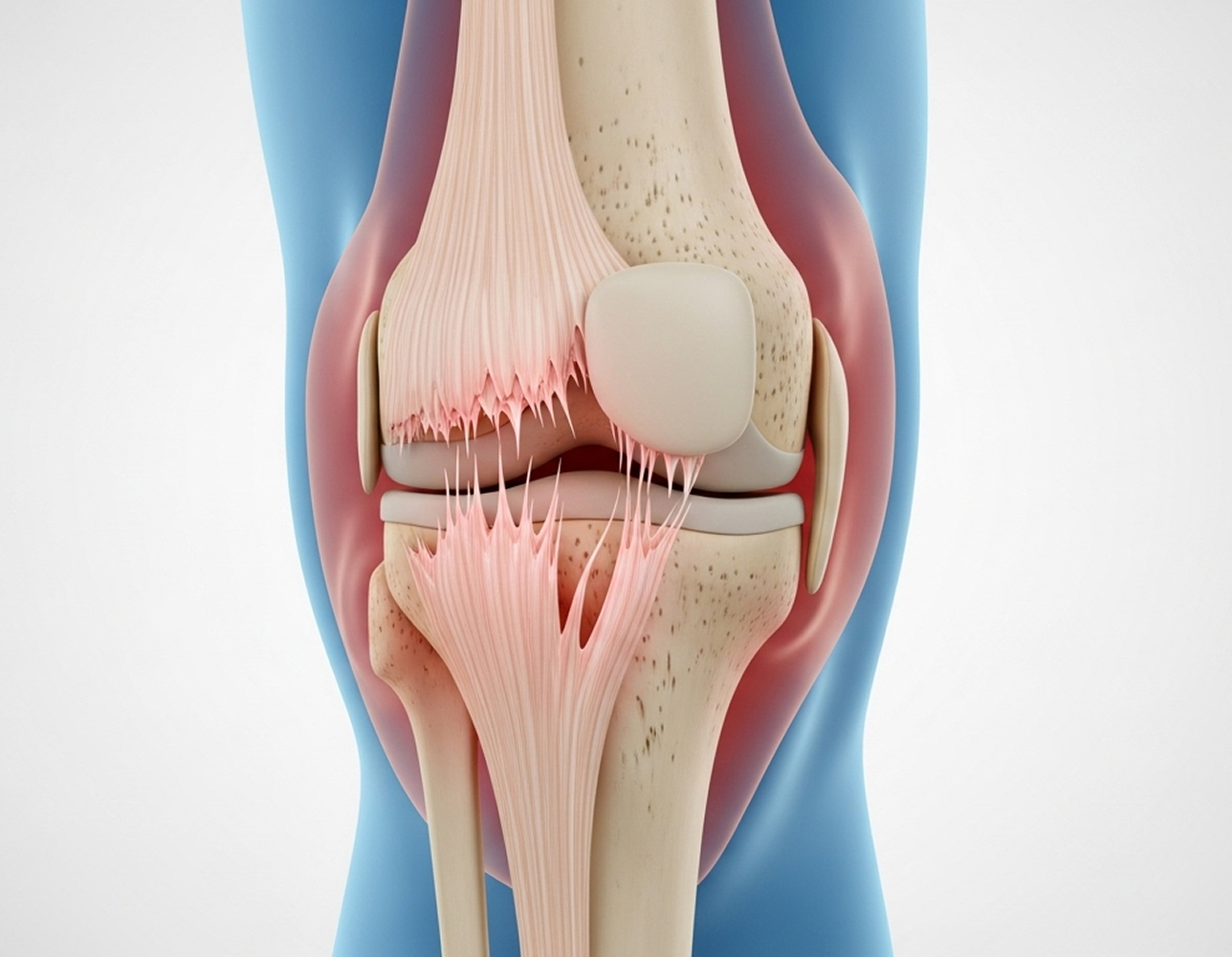
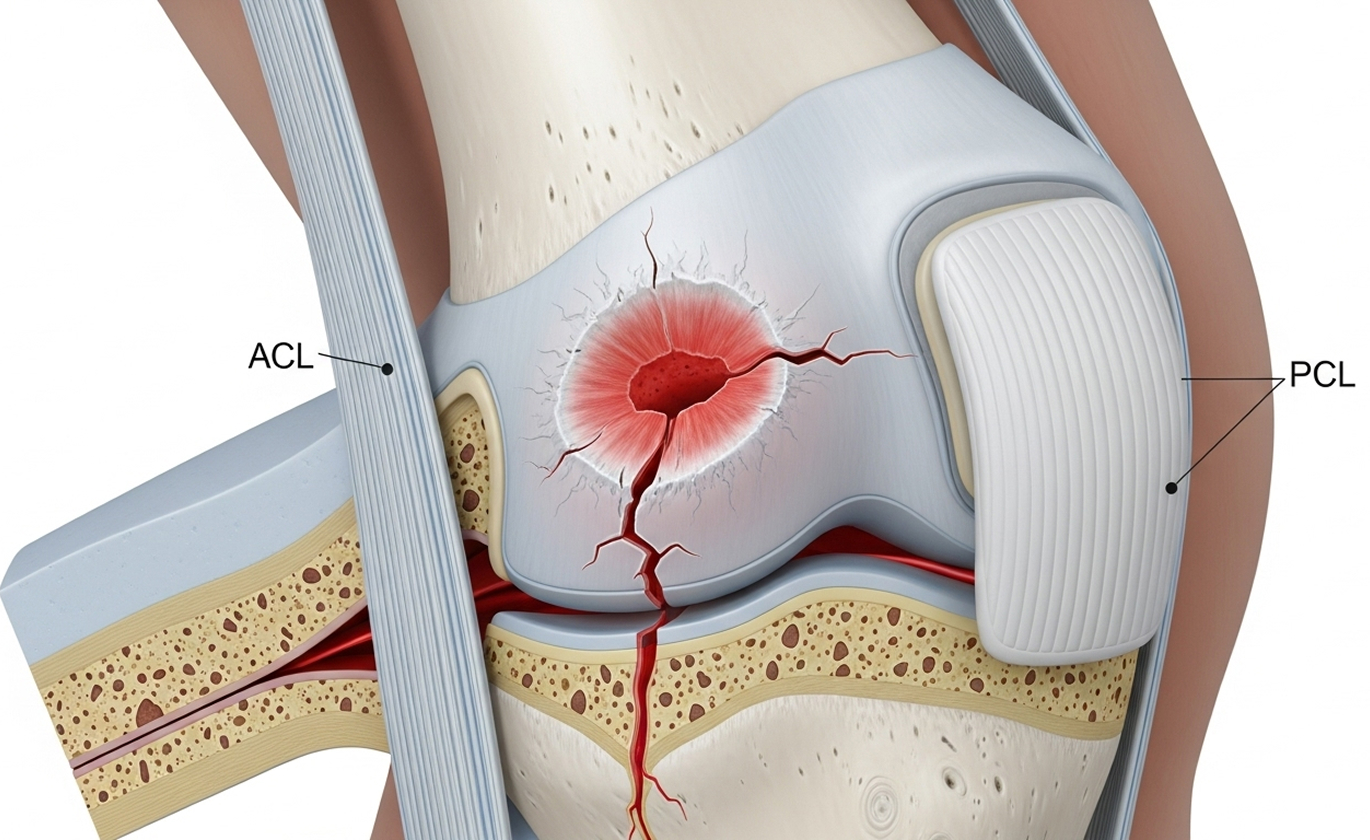
An osteochondral injury involves damage to both the articular cartilage and the underlying bone in a joint, most commonly the knee. Think of articular cartilage as the smooth, white tissue that caps the ends of your bones within a joint, allowing them to glide frictionlessly. Beneath this cartilage lies the subchondral bone, which provides crucial support.
This type of cartilage bone injury knee is more complex than damage limited only to the cartilage surface because it affects this integrated cartilage-bone unit. The term 'osteochondral' itself tells the story: 'osteo' refers to bone, and 'chondral' refers to cartilage.
Doctors classify osteochondral injuries based on several factors, including the stability of the fragment and its size. This helps guide osteochondral defect treatment.



When conservative treatment isn't appropriate or hasn't succeeded, or if the injury is unstable or displaced, surgery offers various options for osteochondral defect treatment and knee cartilage repair. My approach is always evidence-based, considering the specifics of your injury and your goals.
This is often a first-line treatment for small to medium-sized defects (less than 2cm²). Performed arthroscopically, small holes are created in the exposed subchondral bone at the base of the defect. This stimulates bleeding and the formation of a clot rich in marrow cells, which eventually forms a type of scar cartilage called fibrocartilage.
Microfracture is a single-stage procedure with relatively low cost and complication rates. Good short-term results (2-5 years) are seen in 60-80% of patients. However, fibrocartilage is less durable than the original hyaline cartilage and tends to wear down over 5-10 years.
Suitable for medium-sized defects (1-2.5cm²) in younger, active patients. This procedure involves harvesting small cylindrical plugs of healthy cartilage and bone from a non-weight-bearing area of your own knee (autograft). These plugs are then transferred and press-fitted into the defect site, creating a mosaic-like surface.
The main advantage of OATS is that it restores the defect with your own hyaline cartilage, offering good long-term durability (often 10 years or more). Success rates are generally high, around 75-90% good outcomes at 5-10 years. Limitations include the amount of graft available from the donor site and potential pain or issues at the harvest site.
ACI is typically reserved for larger defects (greater than 2cm²) or situations where other surgeries have failed, usually in younger patients (under 40). It's a two-stage procedure:
ACI can treat large defects (up to 10cm²) and achieves good long-term outcomes (70-85% at 10+ years). However, it involves two surgeries, is expensive, has limited public funding in Australia, and requires prolonged rehabilitation (12-18 months).
Used for very large defects (often >2.5-3cm²), particularly those with significant underlying bone loss, or as a revision option after other failed procedures. This involves transplanting a size-matched graft of cartilage and bone harvested from a deceased donor (allograft). It's a single-stage procedure.
Advantages include the ability to treat very large defects without donor site issues. Disadvantages include limited graft availability, the potential for disease transmission (though rigorously screened), and a risk of graft rejection or failure over time (10-25% at 5-10 years). Graft survival rates are around 65-85% at 10 years.
Returning to sport after knee cartilage repair depends on the procedure, defect size, sport type, and individual recovery.
Treating osteochondral injuries requires careful evaluation and a tailored approach. As a fellowship-trained knee subspecialist, I provide comprehensive assessment through clinical examination and detailed review of your imaging (X-ray and MRI). When necessary, diagnostic arthroscopy allows direct visualisation.
My treatment recommendations are always based on the best available evidence, considering the specifics of your osteochondral injury knee, your age, activity level, and long-term goals. Depending on your situation, this may involve a trial of conservative management, arthroscopic surgery for fragment fixation or removal, microfracture, or OATS (mosaicplasty). For very large defects requiring ACI or allograft, I can provide assessment and referral to specialised centres when indicated.
Successful recovery hinges on precise, procedure-specific rehabilitation. I work closely with experienced physiotherapists to ensure you follow the optimal protocol for your surgery, guiding your gradual return to activity. My dual fellowship training (FRCS from the UK and FRACS from Australia) and dedicated focus on knee surgery provide the subspecialist expertise needed to manage these complex injuries effectively.
There isn't a single "best" surgery; the ideal osteochondral defect treatment is highly individualised. Factors influencing the decision include:
If you have symptoms of an osteochondral injury or have been diagnosed with cartilage and bone damage in your knee, I encourage you to schedule a consultation. Together, we can discuss your situation and determine the best treatment path for you.
What to Bring: Please bring your referral letter, all relevant imaging studies (X-rays, CT scans, MRI if performed), and your list of current medications to your consultation.

