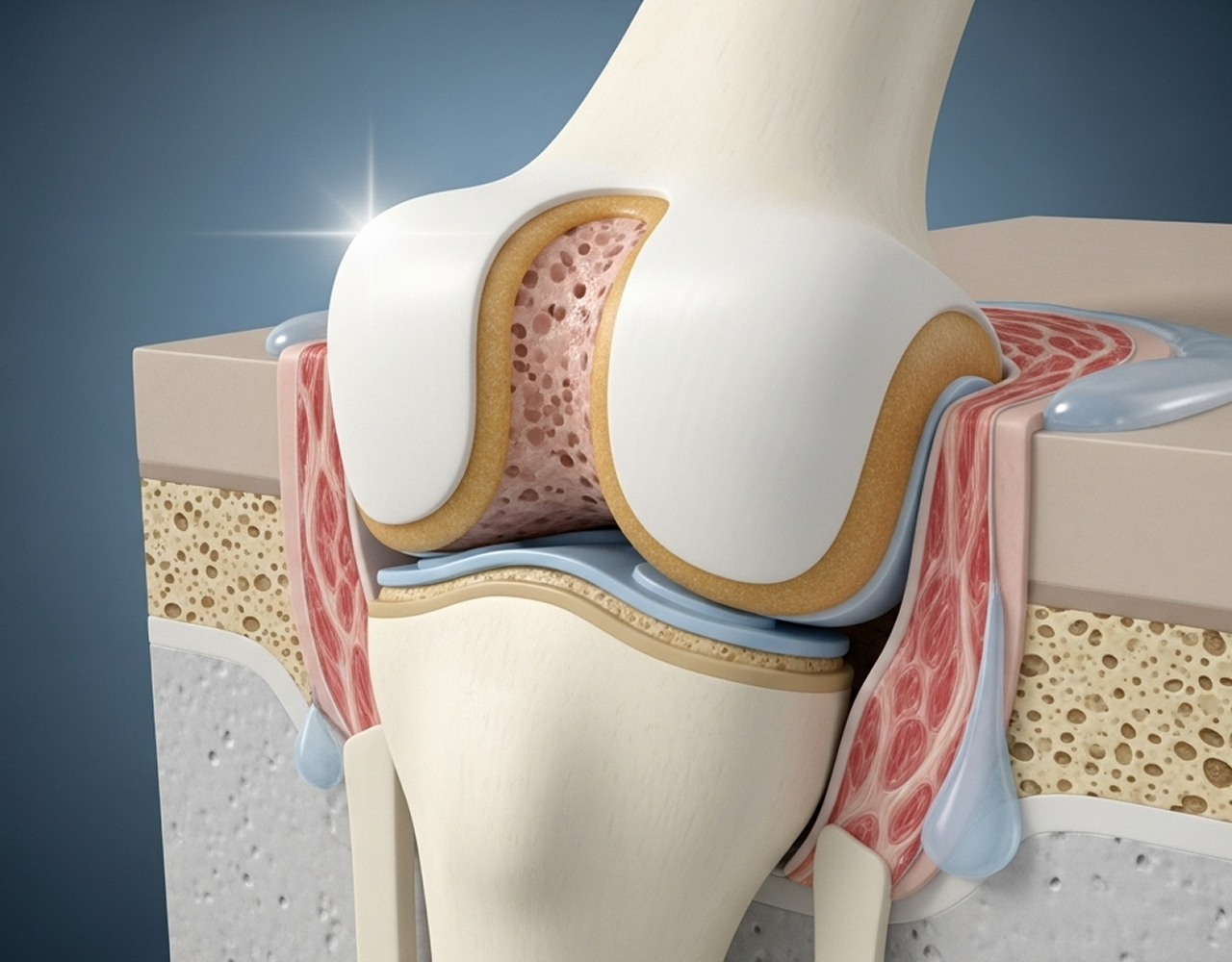
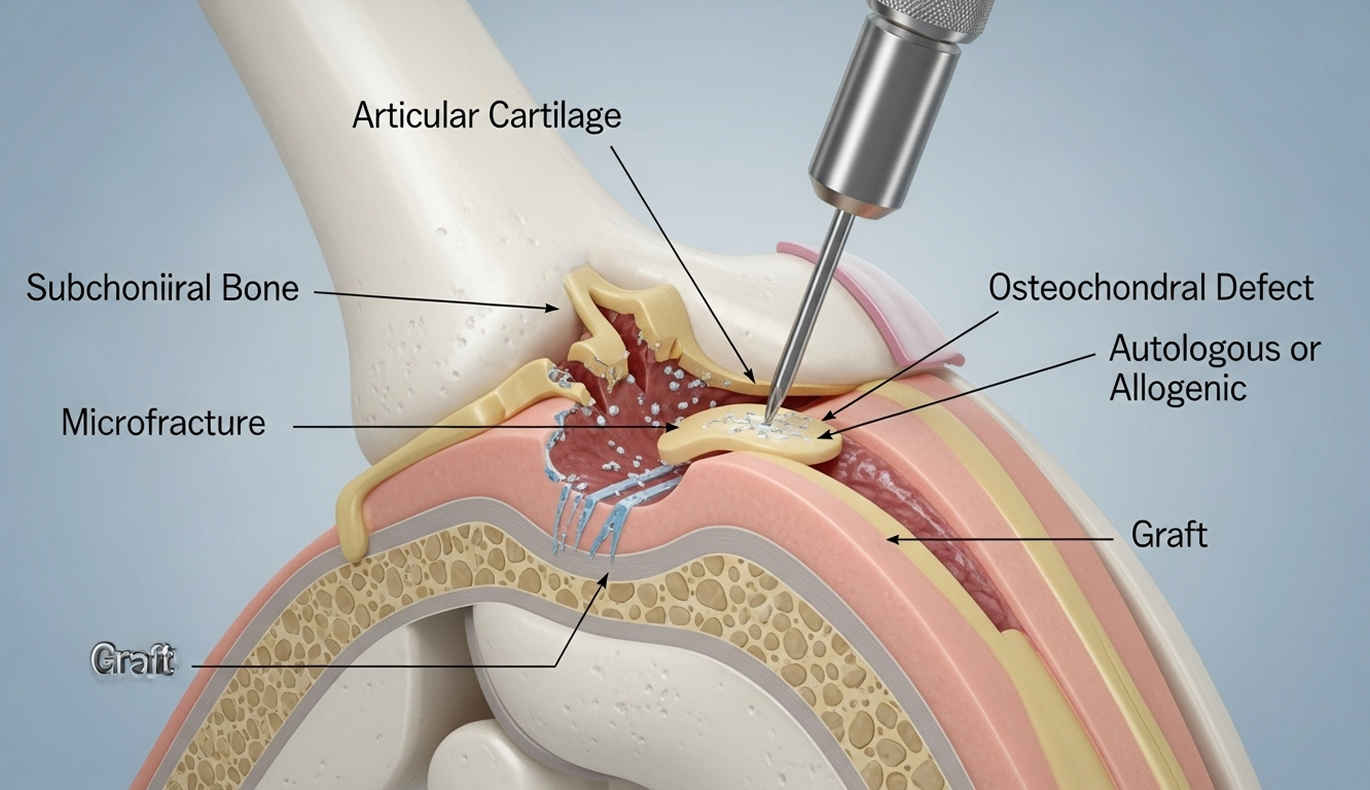
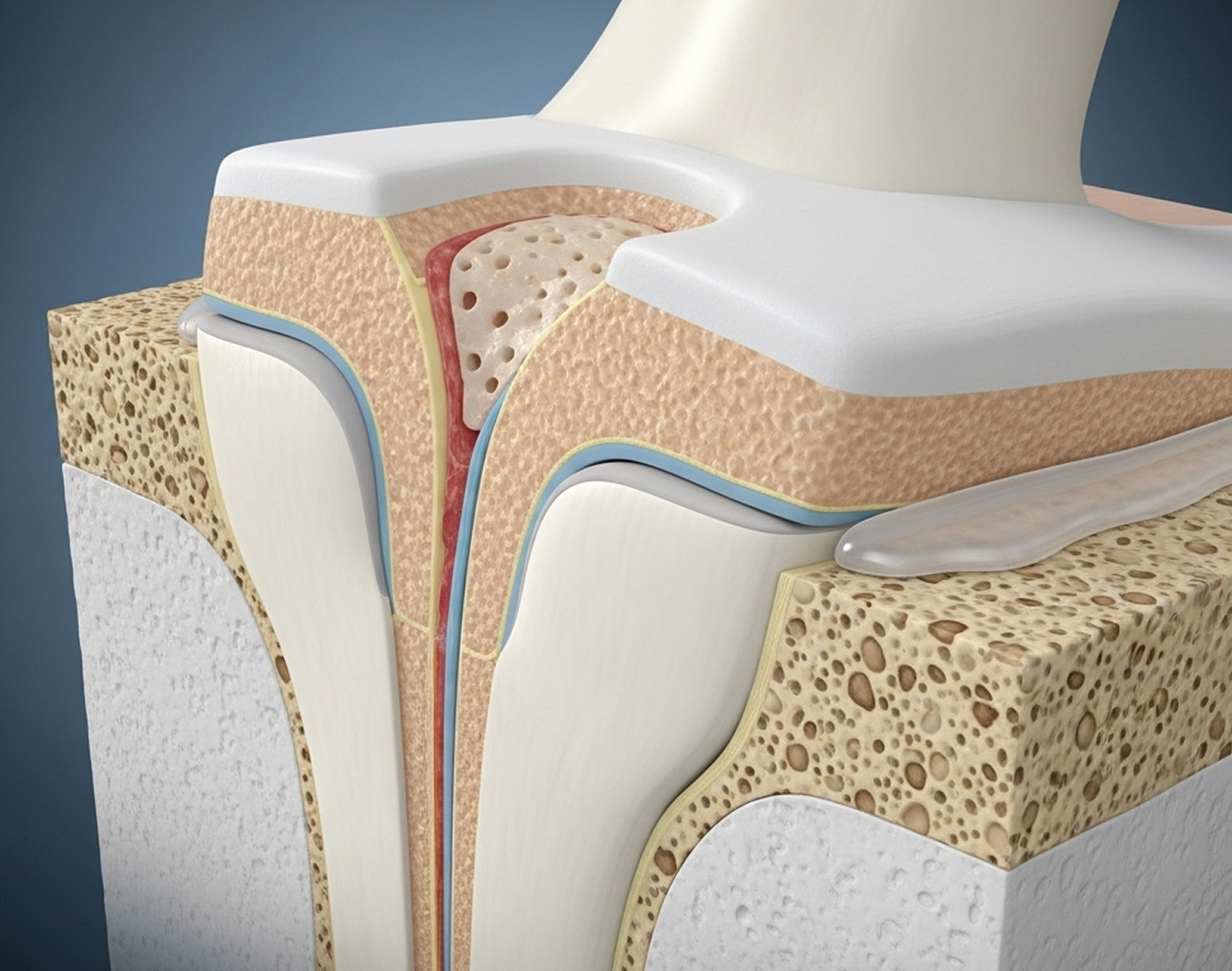
Pure cartilage damage affects only the smooth surface layer (a chondral lesion). An osteochondral lesion involves damage to both the cartilage and the underlying bone. Because the bone has a blood supply, osteochondral lesions sometimes have better potential for healing stimulation (like microfracture) compared to isolated cartilage damage.
Articular cartilage has very poor self-healing ability due to its lack of blood supply. Small, stable defects might not worsen, but they rarely fill in with new, healthy cartilage. Surgery aims to either stimulate a repair response or replace the damaged tissue.
Surgery is often recommended if you have persistent pain or swelling despite non-surgical treatment for 3-6 months, mechanical symptoms like catching or locking, large or unstable lesions seen on MRI, or if your activity goals are limited by the lesion. Small, stable lesions, especially in growing adolescents, might be managed non-surgically first with close monitoring.
There isn't one single "best" treatment. The ideal technique depends heavily on the lesion's size, depth, location, and stability, as well as your age and activity level. Microfracture is common for smaller defects, OATS for medium defects in active people, and fragment fixation for suitable OCD lesions. Dr Allom will discuss the most appropriate evidence-based option for you.
Return-to-sport timelines vary widely depending on the procedure performed and the demands of your sport:
An osteochondral lesion does increase the long-term risk of developing arthritis in that joint. Surgery aims to restore the joint surface, reduce symptoms, and potentially delay the onset or slow the progression of arthritis compared to leaving the defect untreated. It doesn't eliminate the risk entirely, but it often provides many years of improved function.
If you have ongoing knee pain, catching, or swelling, particularly after an injury or if diagnosed with OCD, an expert assessment is the first step. Dr Richard Allom can provide a precise diagnosis and discuss the most effective treatment options tailored to your knee condition and lifestyle goals.
What to Bring: Please bring your referral letter, all relevant imaging studies (X-rays, CT scans, MRI if performed), and your list of current medications to your consultation.

