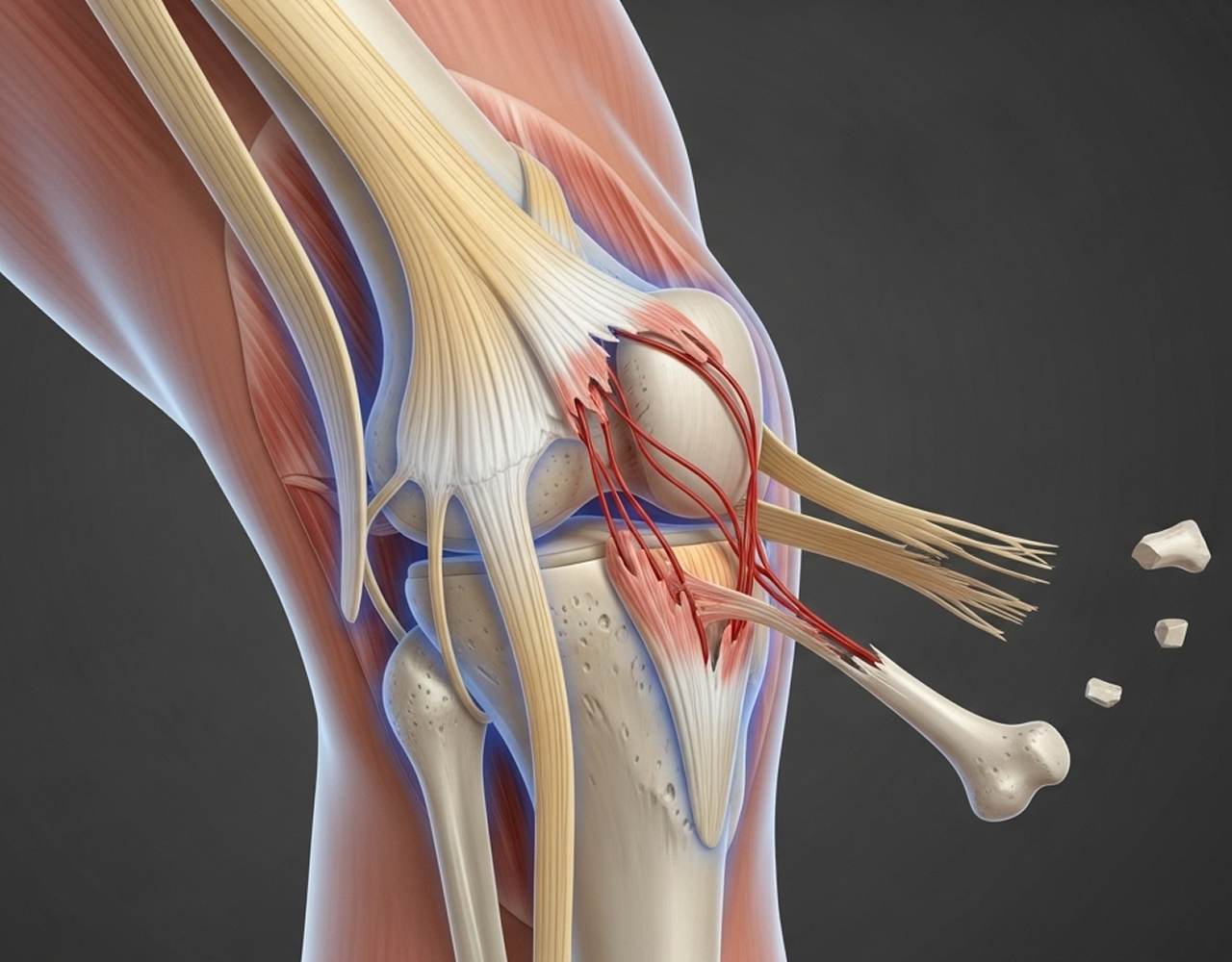
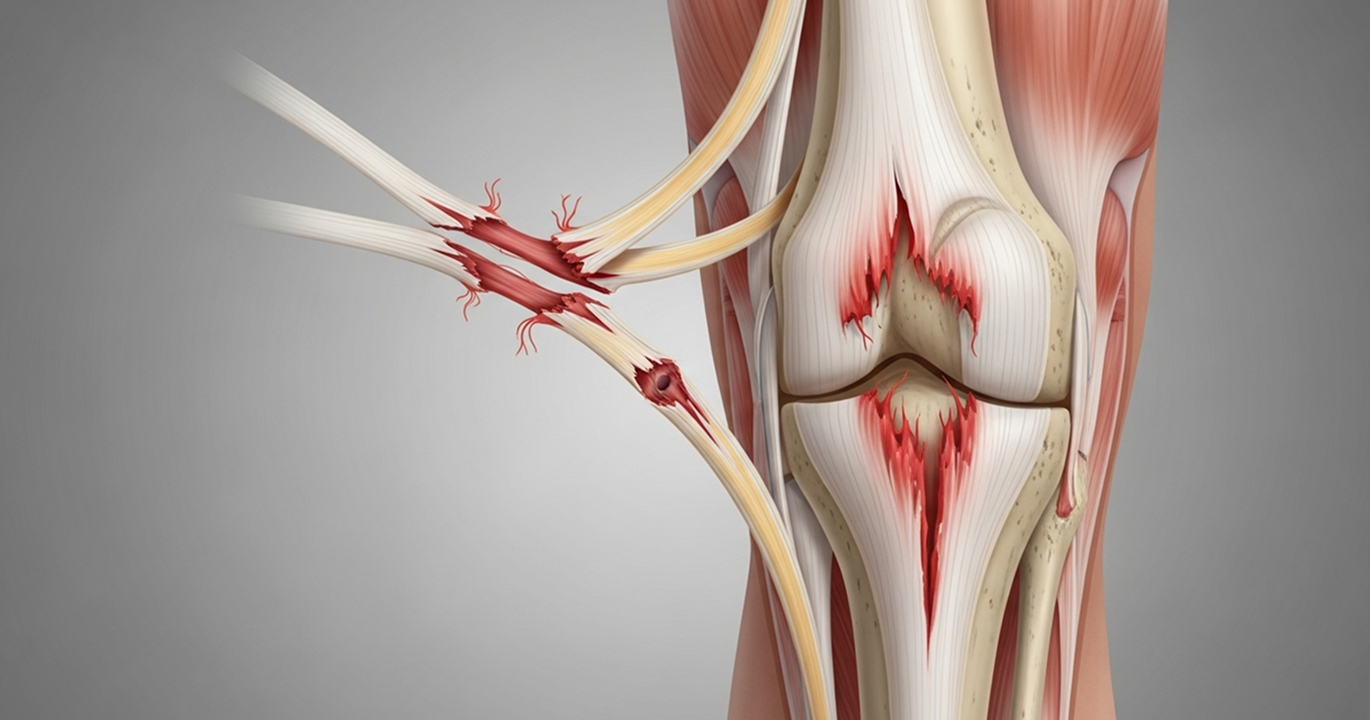
It is crucial to understand: even if your knee looks like it's back in a normal position after a suspected dislocation, severe ligament damage may still be present. Any potential knee dislocation needs urgent assessment by a specialist
Red Flags: Absent or weak pulses, a cold pale foot, severe increasing pain, rapidly expanding bruising, loss of sensation or movement, or a visibly dislocated knee all require immediate action.


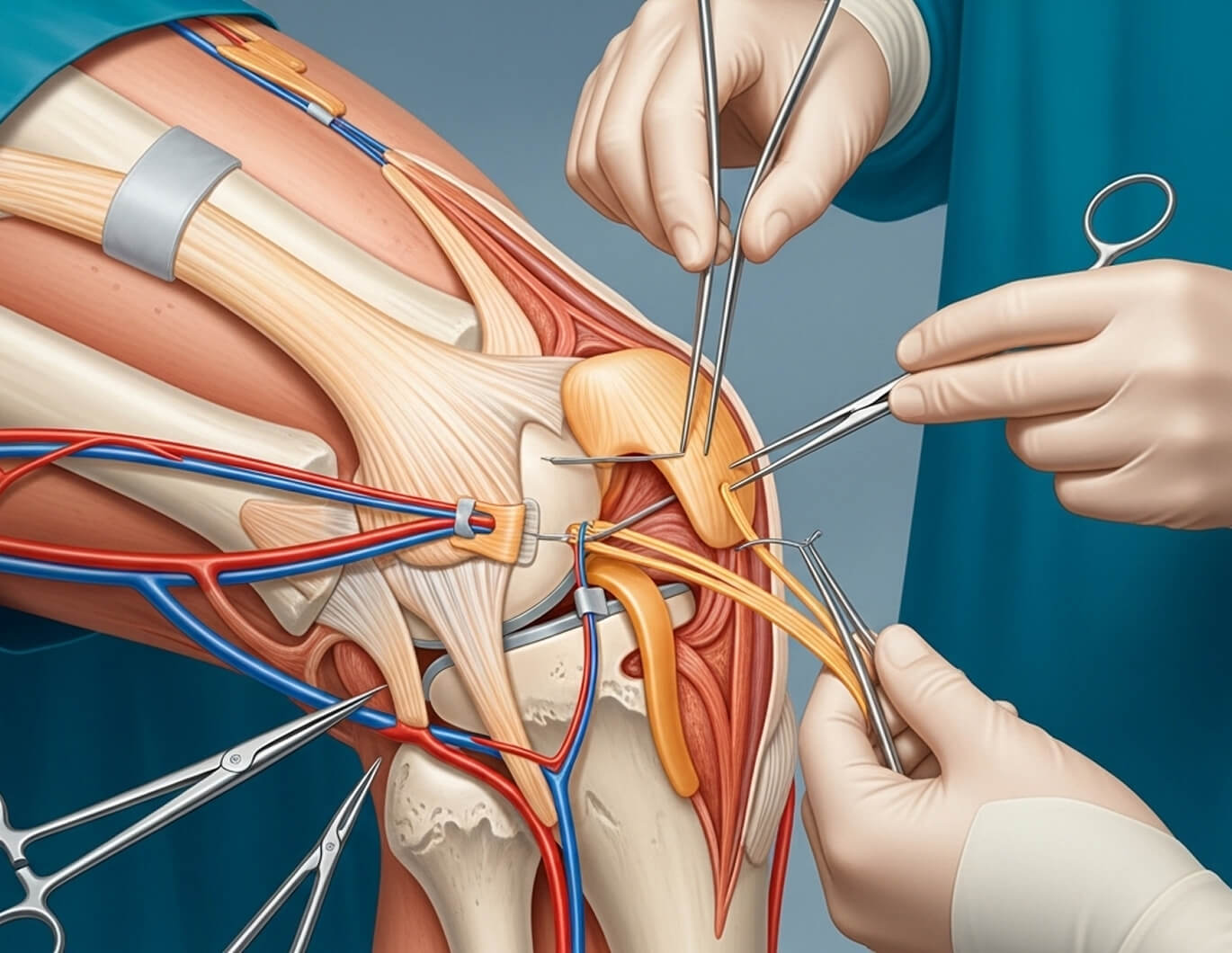
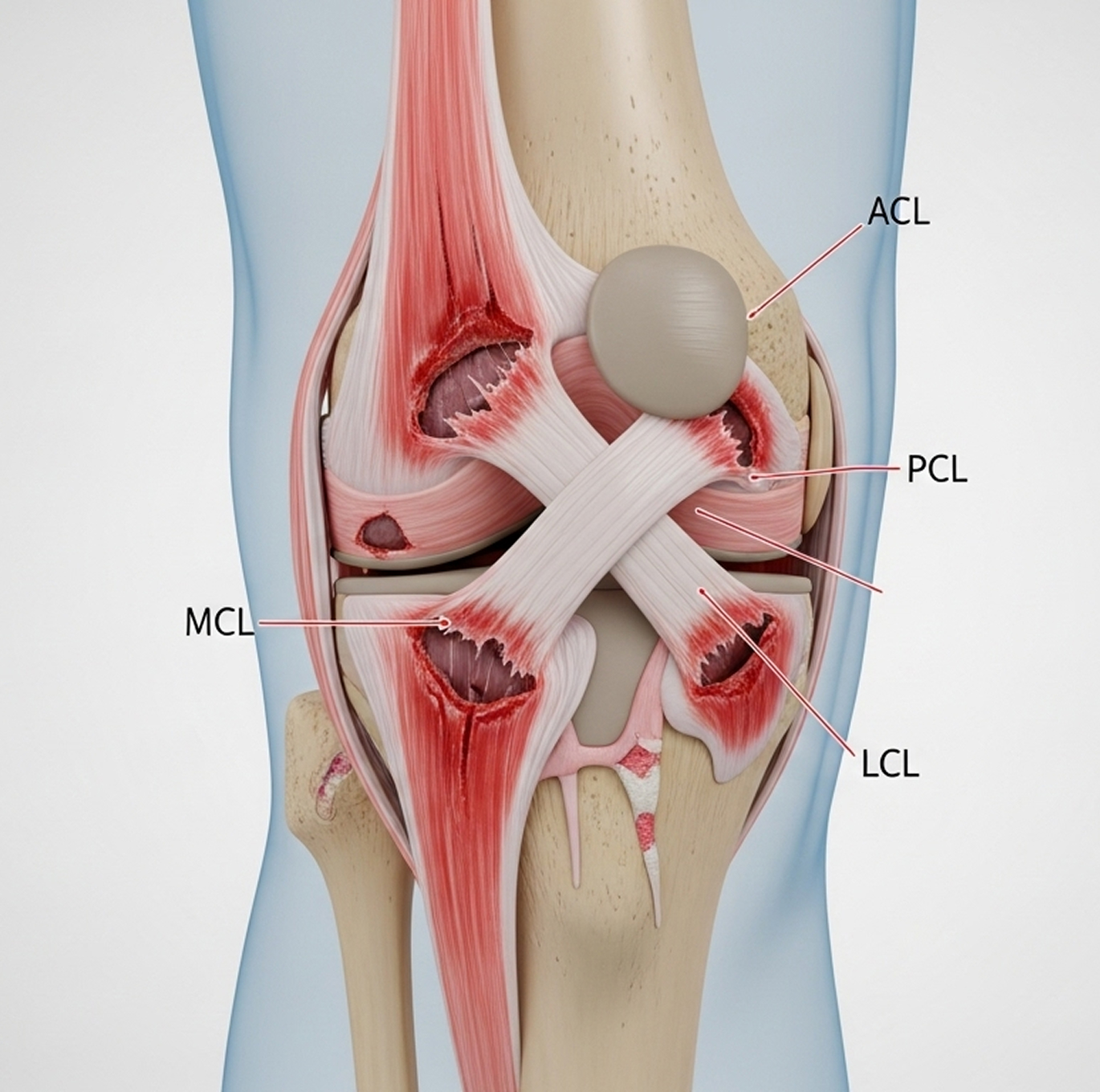
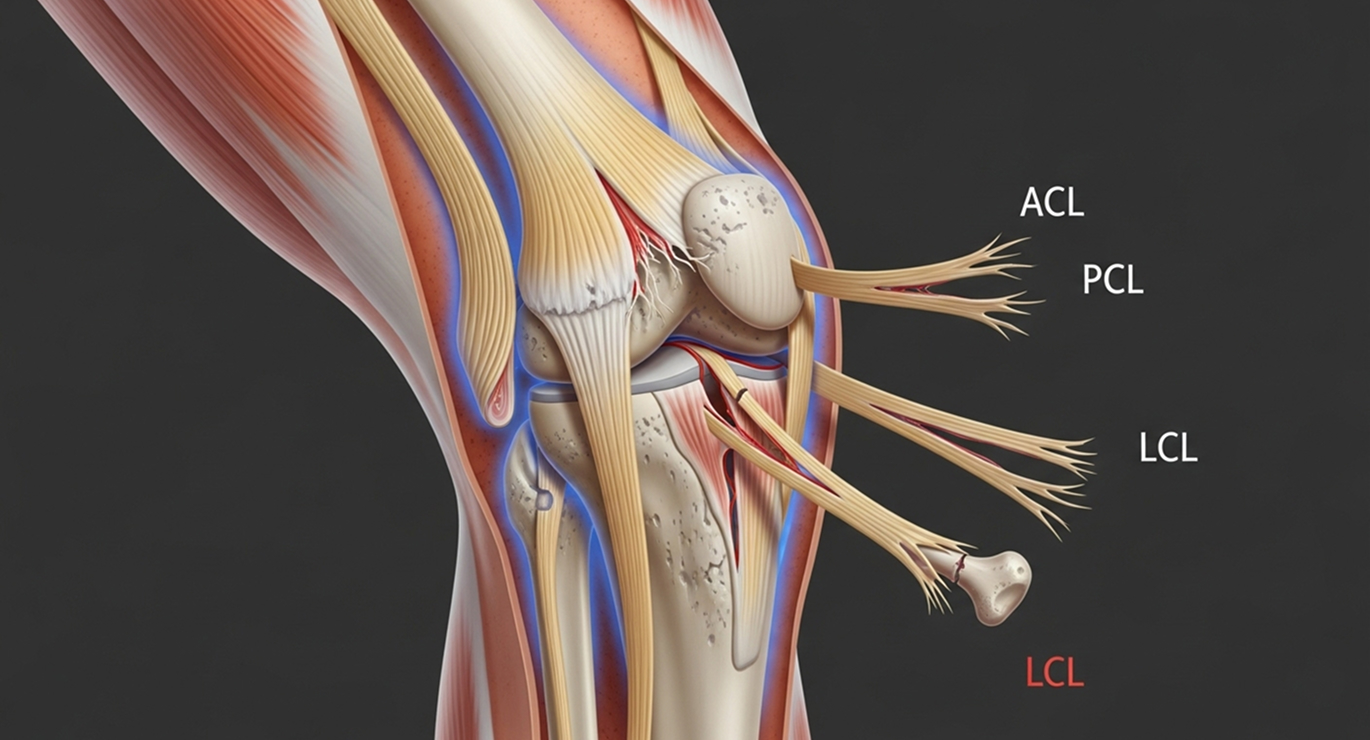
If you have sustained a multiligament knee injury or suspect a knee dislocation, Dr Allom offers subspecialist assessment to discuss your injury and treatment options.
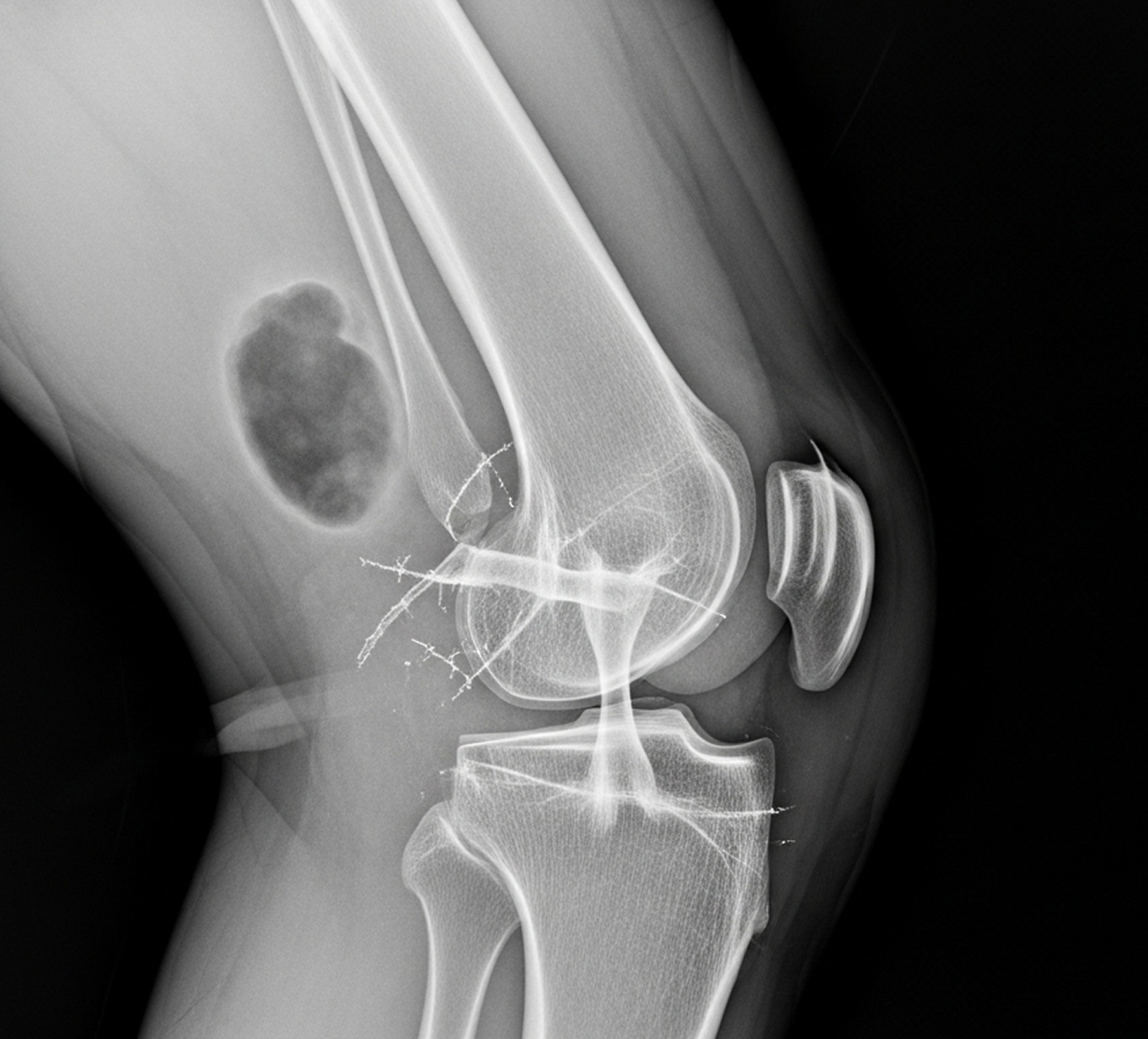
What to Bring: Please bring your referral letter, all relevant imaging studies (X-rays, CT scans, MRI if performed), and your list of current medications to your consultation.

