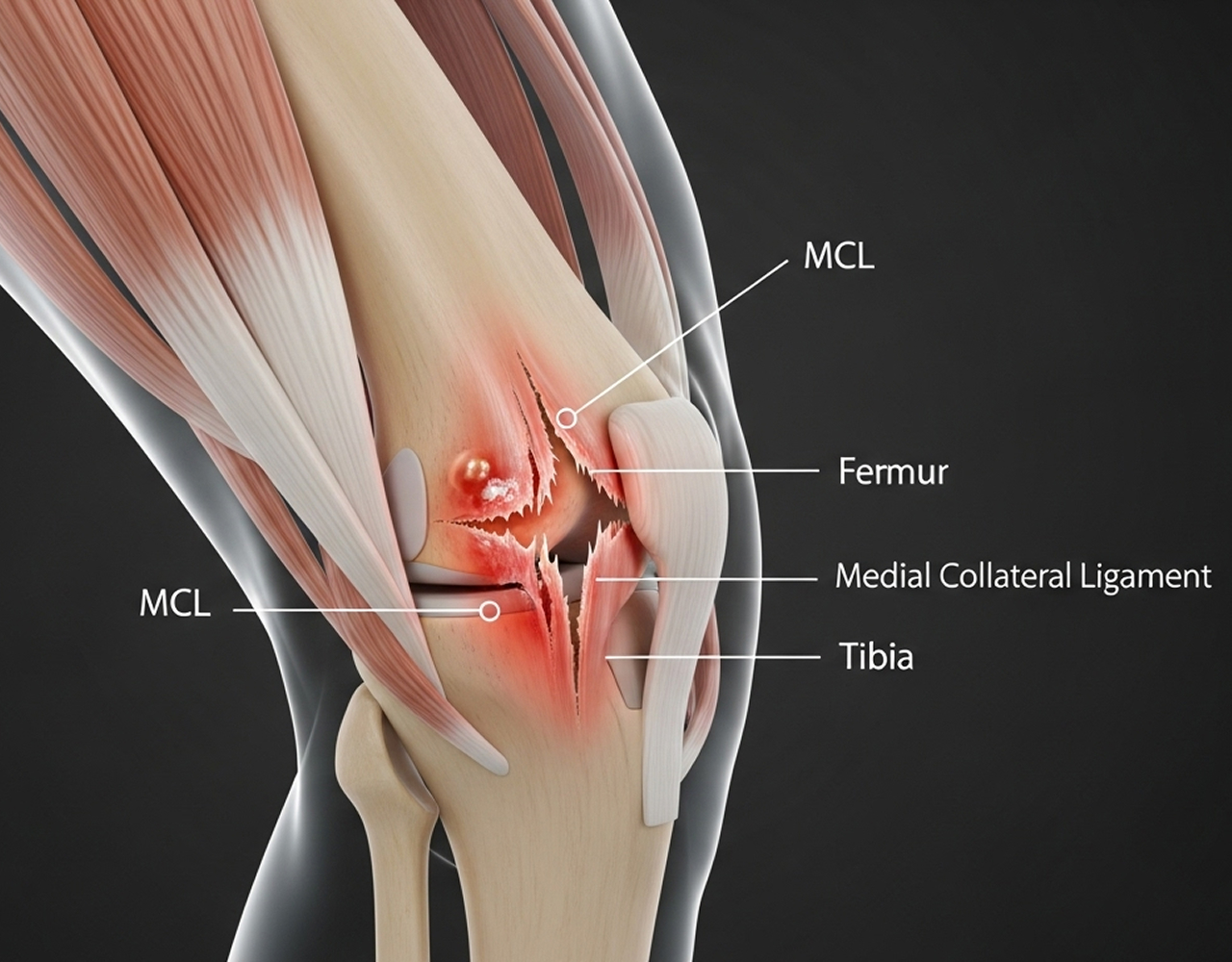
A sharp pain on the inside of your knee after a tackle or a twist. Localised swelling. The feeling that your knee might buckle inward.
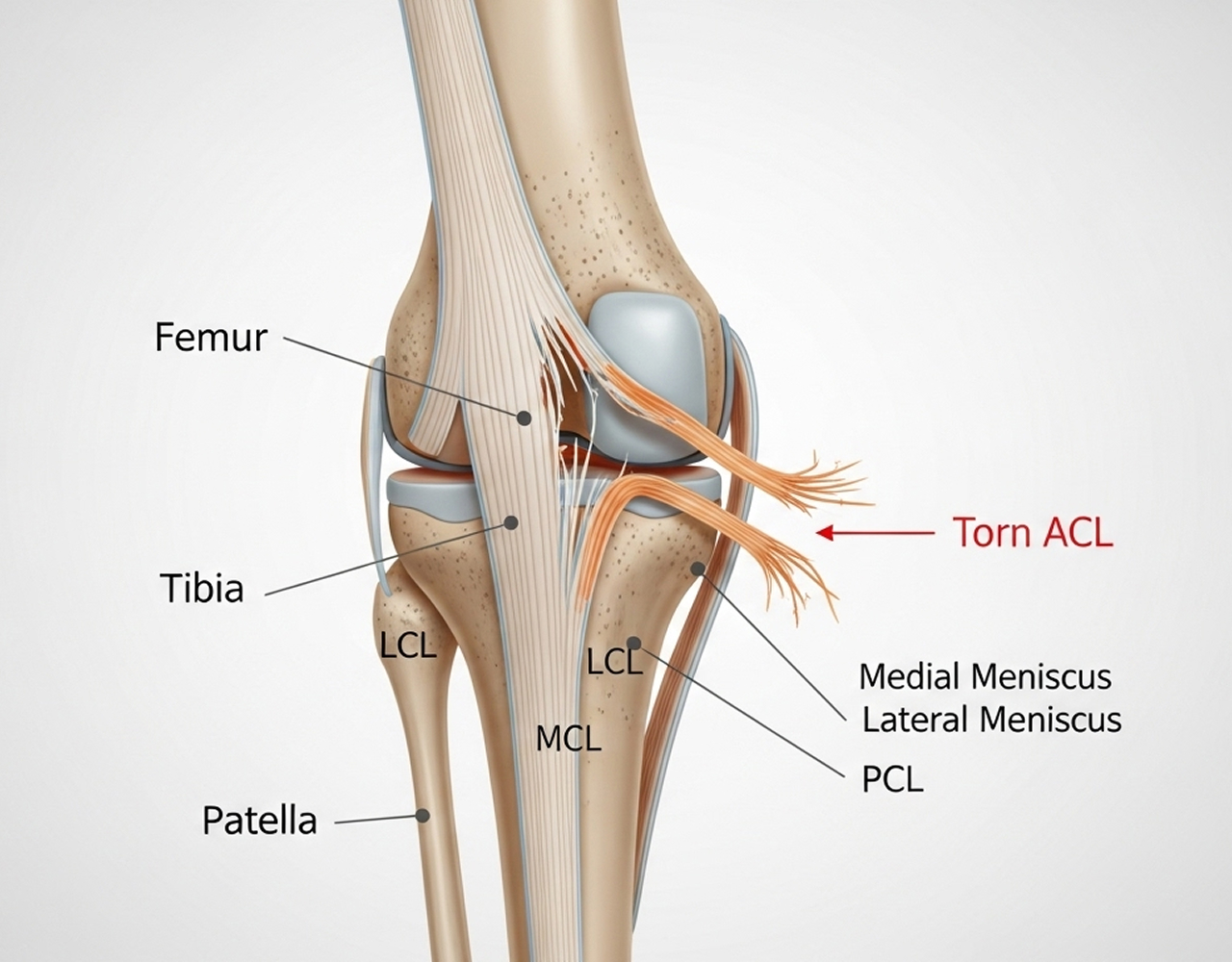
You may have injured your Medial Collateral Ligament (MCL).
While this is the most common knee ligament injury, the news is often better than patients expect. Unlike the ACL, the MCL has a rich blood supply, which means it has a remarkable ability to heal on its own with the right support.
As a knee subspecialist with dual fellowships from the UK and Australia, Dr Richard Allom manages the full spectrum of MCL injuries. From straightforward sprains to complex multi-ligament trauma, he provides the expert guidance needed to ensure your knee heals in a stable position.
His priority is ensuring you get the right diagnosis early, so you don't spend weeks in a brace if you don't need to, or miss a more serious injury that requires attention.
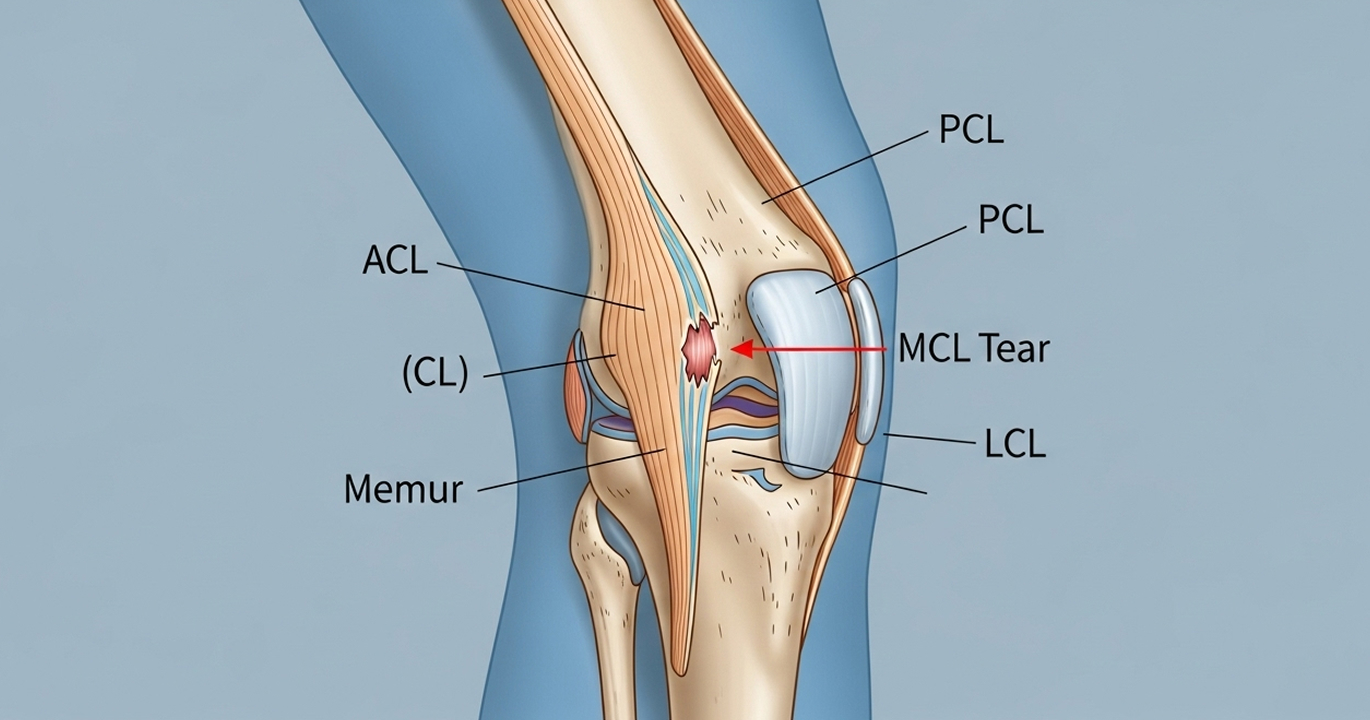
Getting the diagnosis right is critical because MCL tears often happen alongside other injuries, such as ACL tears or meniscus damage.
Dr Allom will conduct a thorough physical examination at his clinics in Campbelltown, Liverpool, Gledswood Hills, Taree, or Forster. He will perform specific stress tests to check the "gapping" of your knee joint, which helps determine the grade of the tear.
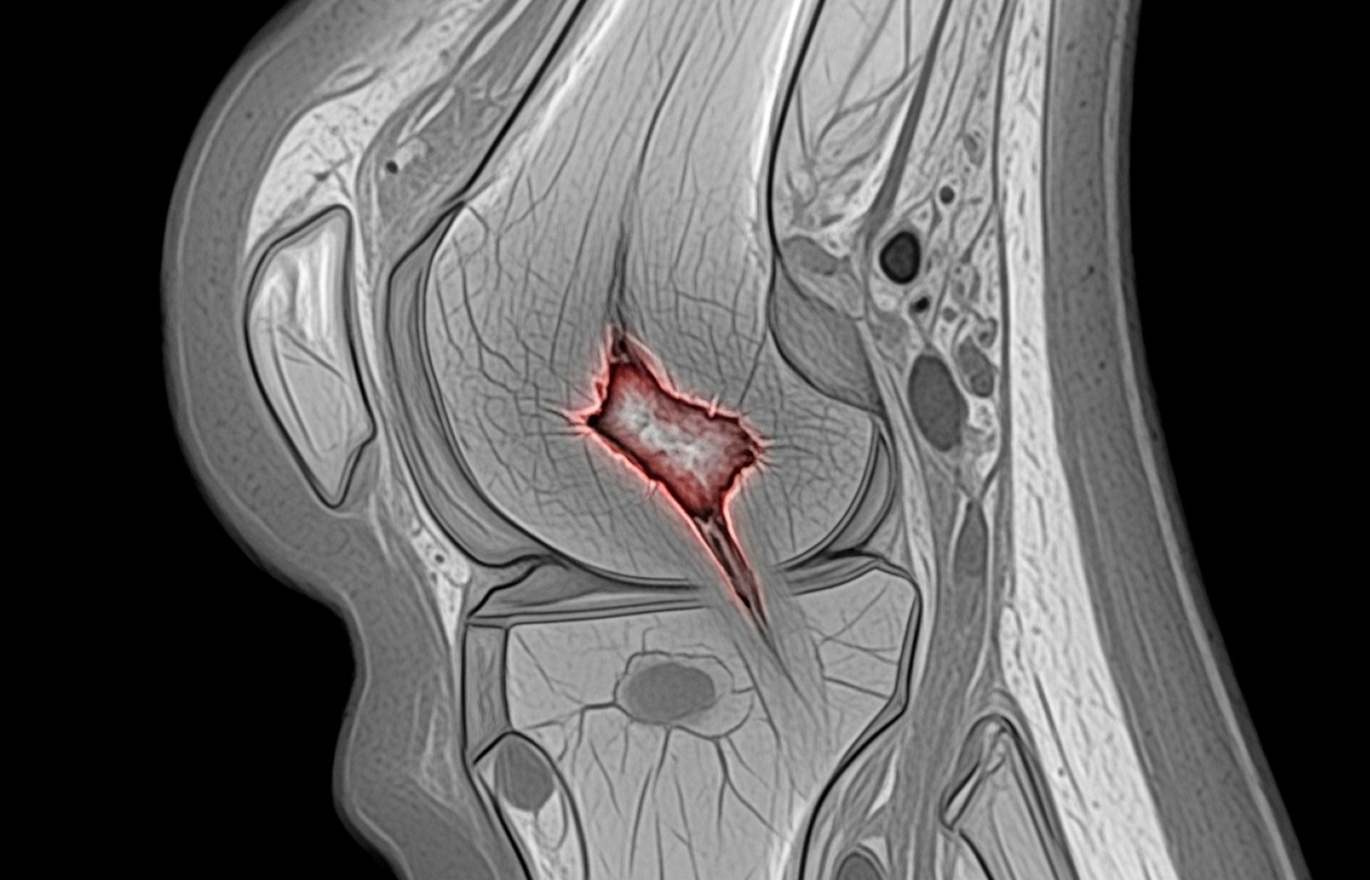
To confirm the diagnosis, he will refer you for an MRI scan
While an X-ray checks for bone fractures, an MRI is essential for seeing the severity of the ligament tear and checking if the ligament has pulled a piece of bone off (an avulsion), which might change your treatment plan.

Dr Allom combines subspecialist expertise with a practical, patient-focused approach. With experience working in major trauma centres in London and Sydney, he is skilled in managing complex knee trauma.
He holds a Master’s Degree in Surgery and is a Fellow of both the Royal Australasian College of Surgeons and the Royal College of Surgeons of England.
He is committed to avoiding unnecessary surgery. He ensures you understand your injury and your rehabilitation protocol so you can play an active role in your recovery.
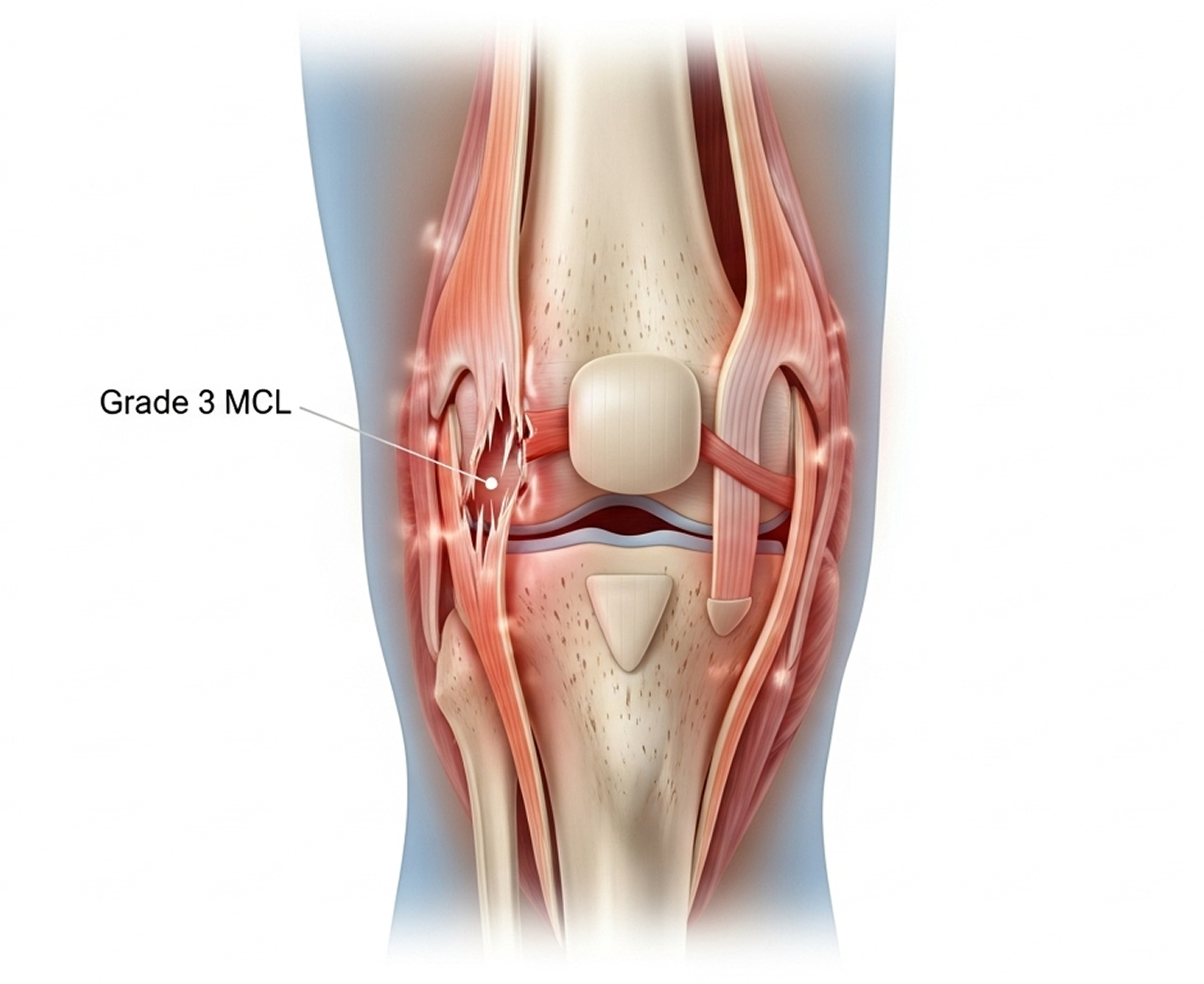
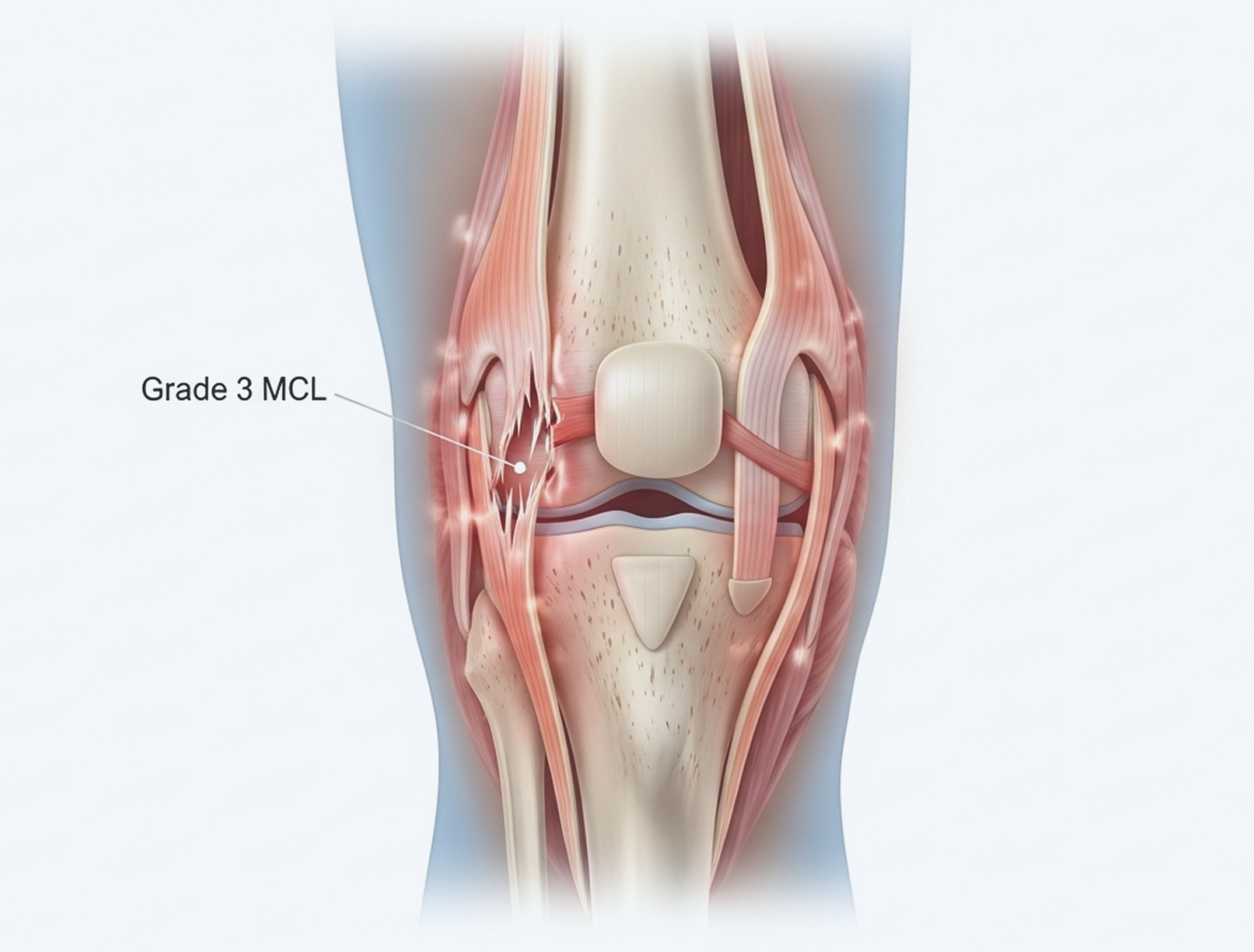
"The MCL is unique. It’s the one ligament in the knee that really wants to heal. My job with an MCL injury is usually to guide the ship, making sure you’re in the right brace, moving at the right time, and not rushing back too early. We generally only talk about surgery if the ligament has pulled off the bone or if the knee stays loose after months of rehab. For 90% of my patients, we can get you back to sport with a good brace and a good physio."

In most cases, no. Unlike the ACL, a complete Grade III MCL tear can heal effectively with a hinged knee brace. Surgery is usually only considered if there is persistent instability after conservative treatment or if multiple ligaments are damaged.
Yes, most patients can weight-bear immediately, though it may be painful. For higher-grade tears, Dr Allom may recommend crutches for 1 to 2 weeks to offload the joint and allow the initial healing process to begin. Early controlled movement is actually beneficial for healing.
Isolated MCL injuries rarely lead to arthritis if they are rehabilitated correctly. The risk of arthritis increases if the MCL injury occurred alongside damage to the meniscus or cartilage, or if the knee remains chronically unstable over a long period.
It is common to tear the ACL and MCL together during a significant sporting impact. If your knee feels extremely unstable, or if there was a loud 'pop' and massive swelling within the joint, you may have a combined injury. An MRI scan is the only way to confirm this definitively.
If you have suffered a knee injury and want to know if it will heal on its own or requires intervention, a specialist assessment provides clarity.
What to Bring: Please bring your referral letter, all relevant imaging studies (X-rays, CT scans, MRI if performed), and your list of current medications to your consultation.