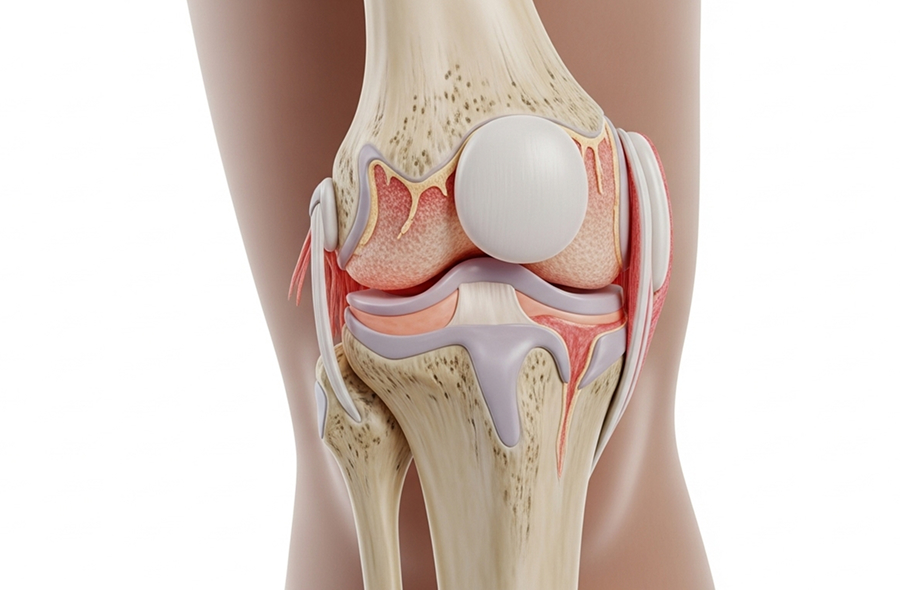
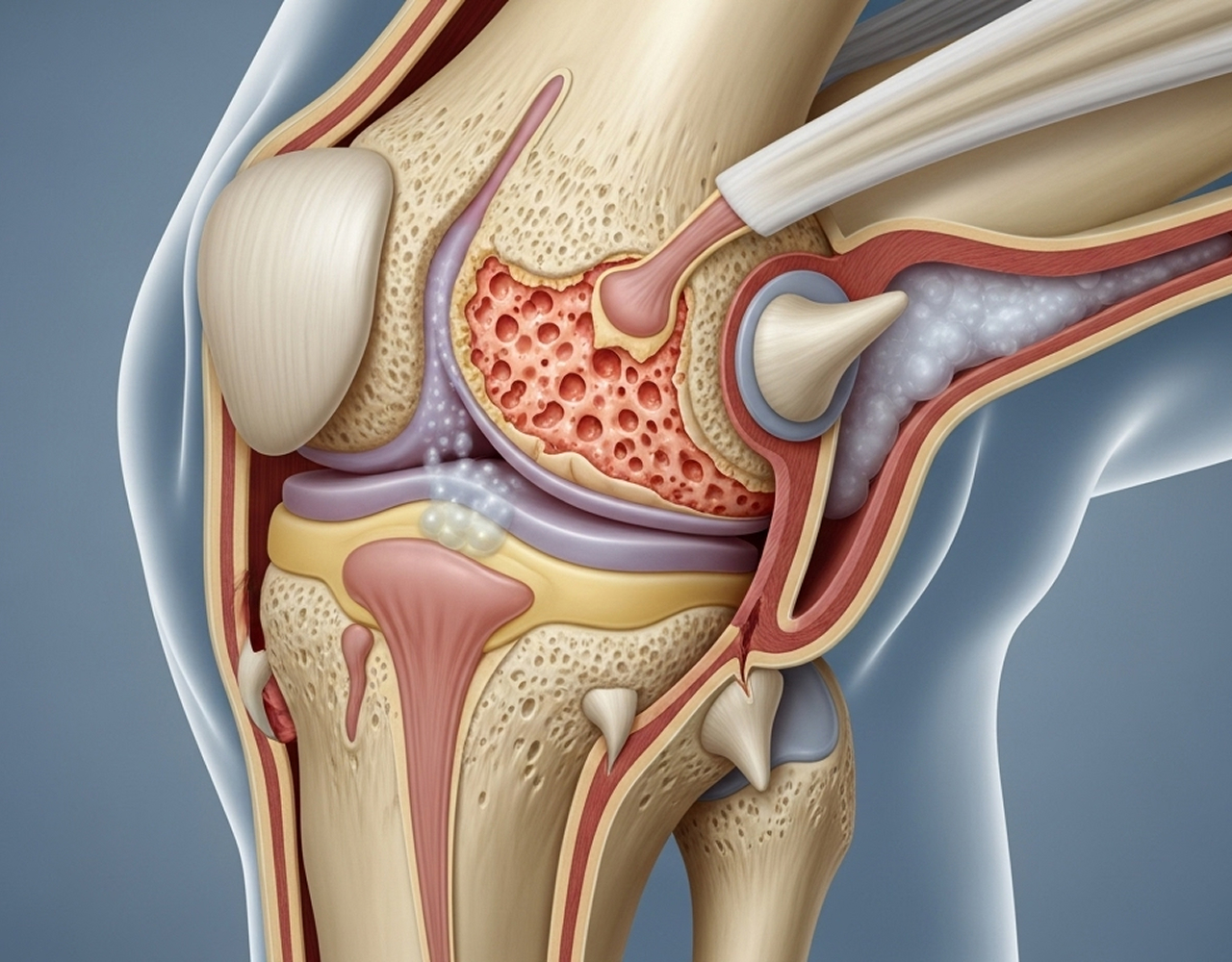
Rheumatoid arthritis typically affects knees in a symmetrical pattern with diffuse joint inflammation, synovial thickening causing persistent swelling, Baker's cyst formation, and ligament laxity from chronic inflammation.

Management requires multidisciplinary coordination between rheumatology, orthopaedics, physiotherapy, and occupational therapy.

Research demonstrates 85-90% of RA patients achieve excellent pain relief and quality of life improvement, with implant survival rates comparable to osteoarthritis patients at 10-15 years. Source: The Journal of Bone and Joint Surgery - TKR Outcomes in Rheumatoid Arthritis - 2024.



Managing rheumatoid arthritis affecting the knee requires close collaboration between your rheumatology team and orthopaedic specialist. I work in partnership with your rheumatologist, providing orthopaedic assessment, surgical options discussion, timing surgery around disease activity, and coordinating post-operative care.
"Managing rheumatoid arthritis is a team effort. My role as the orthopaedic specialist is to work closely with your rheumatologist. We focus on controlling the systemic disease first. Surgery, like a total knee replacement, is a powerful tool for pain relief when the joint damage is advanced, but it is only considered after all medical and conservative options have been optimised. RA presents unique challenges, like softer bone and higher infection risks, so my subspecialist training in complex cases and revision surgery is crucial to ensuring a safe and successful outcome."

Continued rheumatology care manages disease-modifying therapy and systemic inflammation, whilst orthopaedic follow-up monitors implants annually and assesses other joints.

Yes. Total knee replacement is safe and effective when performed by experienced subspecialists with appropriate pre-operative optimisation. Whilst RA patients have slightly higher infection risk, meticulous surgical technique and coordinated care minimise complications. Research demonstrates 85-90% report significant improvement.
Some medications require temporary adjustment, particularly biologics. Your rheumatologist coordinates with me to balance infection risk with disease control, creating an individualised medication plan.
No. Surgery treats joint damage but doesn't cure the underlying autoimmune condition. You'll continue requiring rheumatology management for systemic disease control. However, total knee replacement dramatically relieves pain and restores function in the treated knee.
Optimal timing balances symptom severity, functional limitation, and disease control. Surgery is appropriate when pain significantly impacts quality of life, conservative treatments have been exhausted, joint damage is advanced, and systemic RA is well-controlled. I work with your rheumatologist determining the right timing.
Modern implants perform well, with survival rates similar to osteoarthritis at 10-15 years. Positive factors include lighter body weight and lower activity demands. Potential concerns include bone quality and infection risk. With careful patient selection and ongoing medical management, excellent long-term outcomes are achievable.
Infection risk is slightly higher (1-2%) due to immunosuppressive medications, but modern protocols minimise this. Treatment depends on timing: early infections may require washout surgery retaining implants, whilst late infections require two-stage revision. As a subspecialist trained in complex revision surgery, I manage infected replacements requiring advanced techniques.
If rheumatoid arthritis is affecting your knee and conservative management isn't providing adequate relief, I welcome the opportunity to discuss your treatment options.
I welcome patients across South West Sydney and the Mid North Coast seeking expert management of complex knee fractures.
What to Bring: Please bring your referral letter, all relevant imaging studies (X-rays, CT scans, MRI if performed), and your list of current medications to your consultation.