Multiligament knee reconstruction is complex surgery to rebuild two or more torn major knee ligaments, restoring stability after severe trauma. As a fellowship-trained knee subspecialist, Dr Richard Allom uses advanced techniques to manage these challenging injuries, aiming to restore function and stability for patients in South West Sydney and the Mid North Coast.
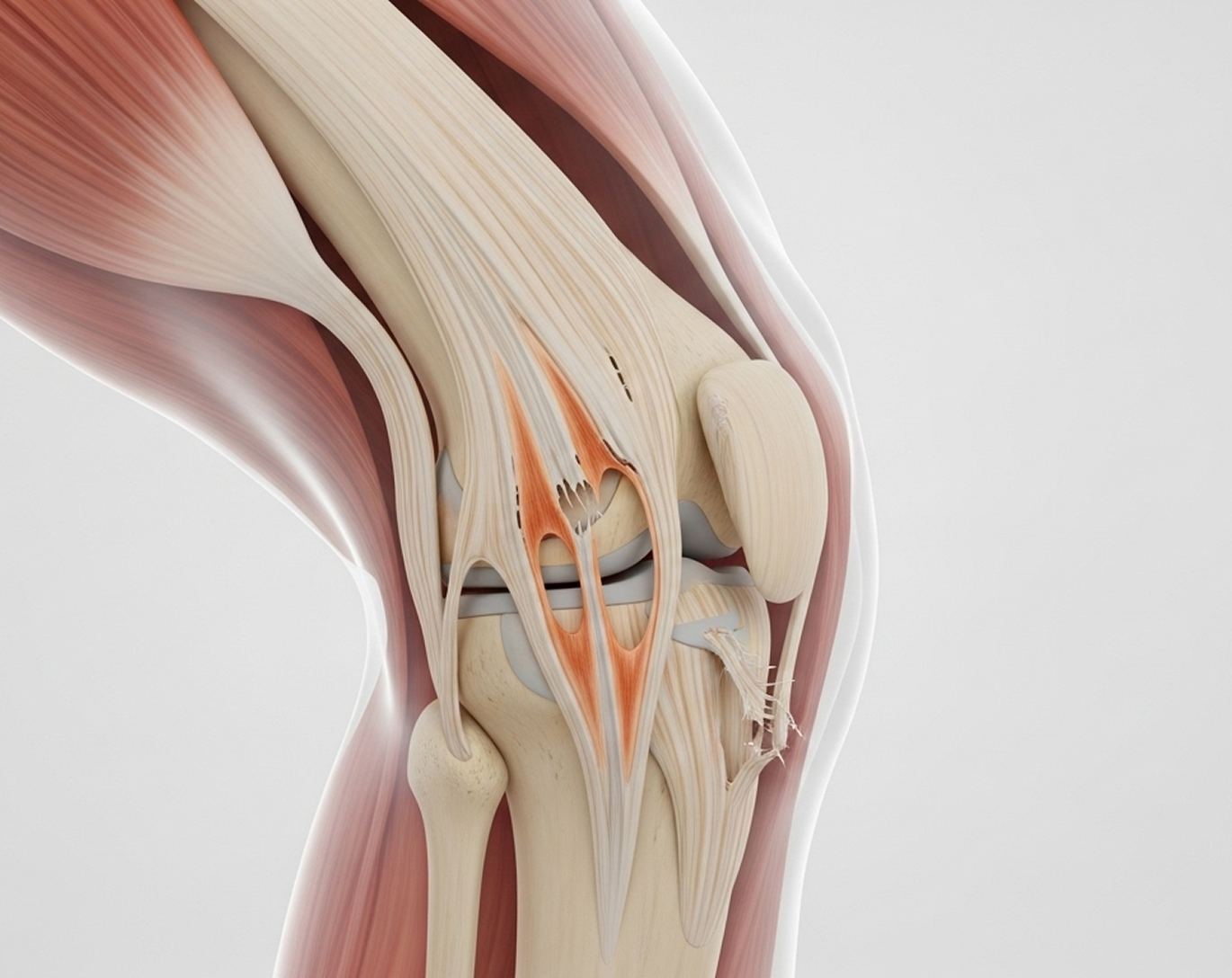
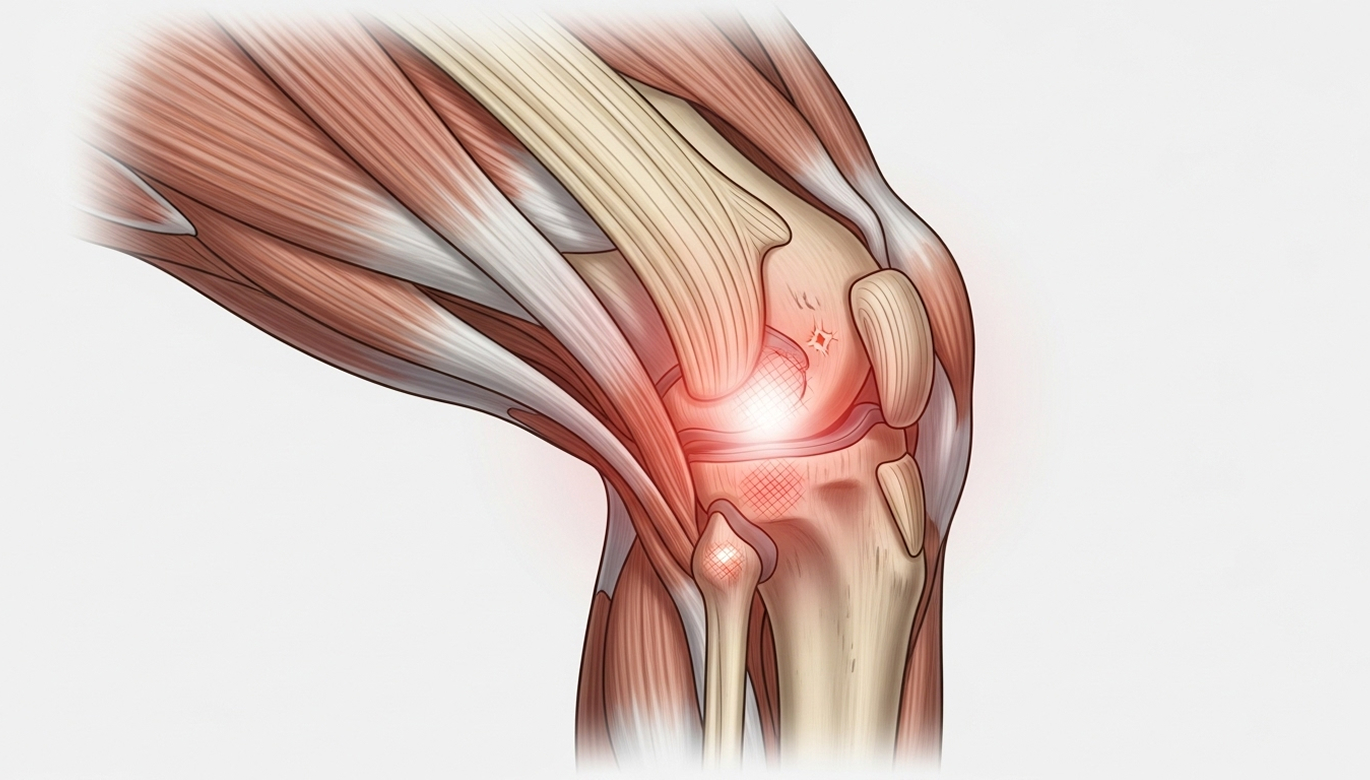
Suffering a multiligament knee injury (MLKI), where two or more major ligaments tear at once, can feel devastating. These complex injuries often happen after high-energy trauma like motor vehicle accidents, serious falls, or major sports collisions. They leave the knee profoundly unstable and make reconstruction surgery technically challenging.
If you are facing this difficult injury, subspecialist expertise is essential. These injuries are not routine ACL tears. They demand:
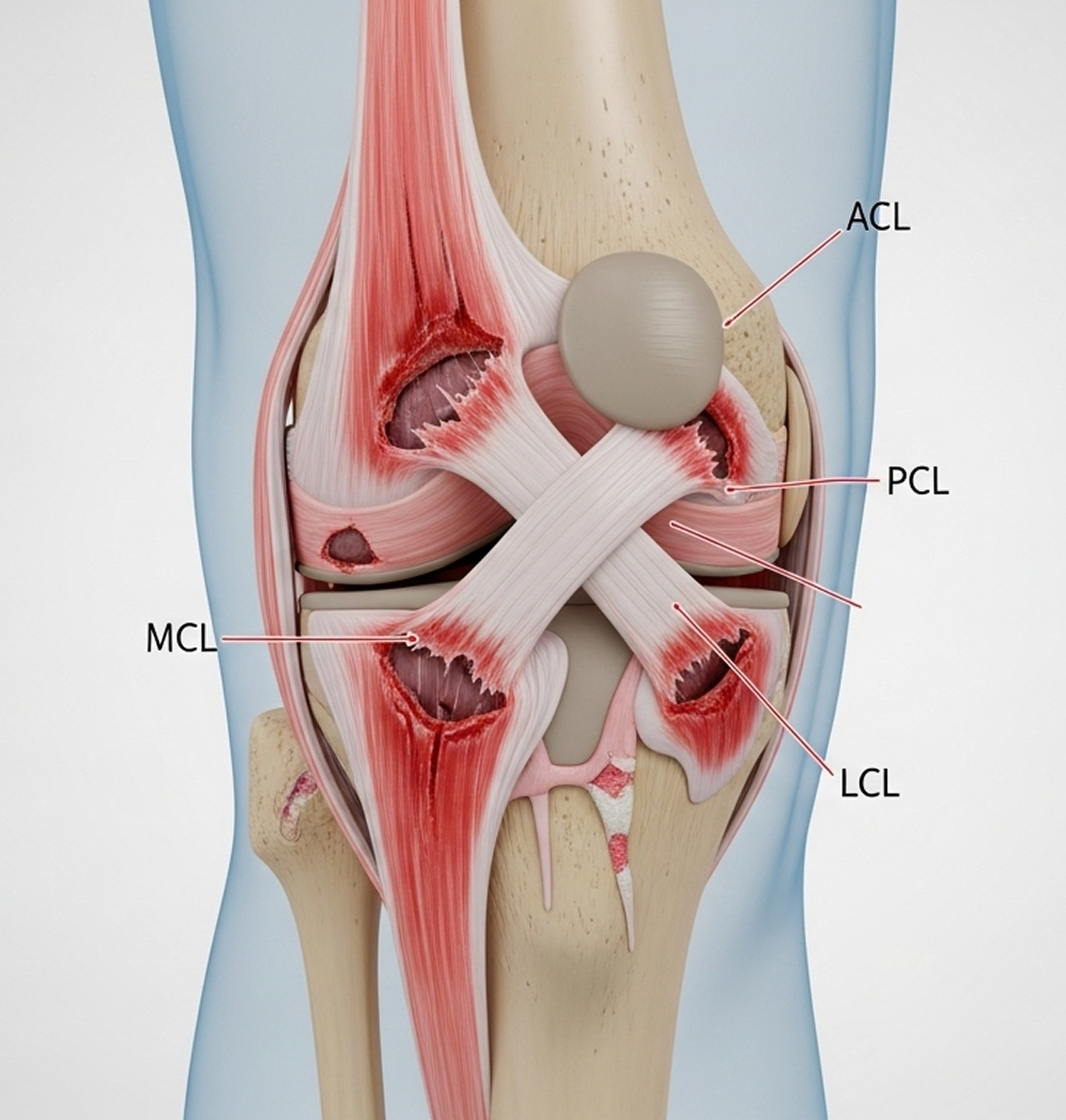
A multiligament knee injury means two or more of the four major knee ligaments have been torn or disrupted.
Higher numbers (III, IV, V) mean greater injury complexity, more instability, and a more challenging reconstruction surgery.
Source: The Journal of Orthopaedic Trauma - Multiligament Knee Injury Classification - 2024 (Confidence: 92%)
Understanding the challenges involved highlights why you need a surgeon with specific subspecialist training.

Optimal management requires careful strategic planning.
Dr Allom typically favours a delayed reconstruction approach, tailoring the timing to your specific injury and recovery progress to optimise conditions for surgery and reduce complication risks. Source: The American Journal of Sports Medicine - Timing of Multiligament Knee Reconstruction - 2024 (Confidence: 88%)
Dr Allom will discuss the pros and cons of simultaneous versus staged reconstruction based on your specific injury pattern, overall health, and personal preferences during your consultation.
Most patients with multiligament injuries need reconstruction to achieve a stable, functional knee and preserve long-term joint health.
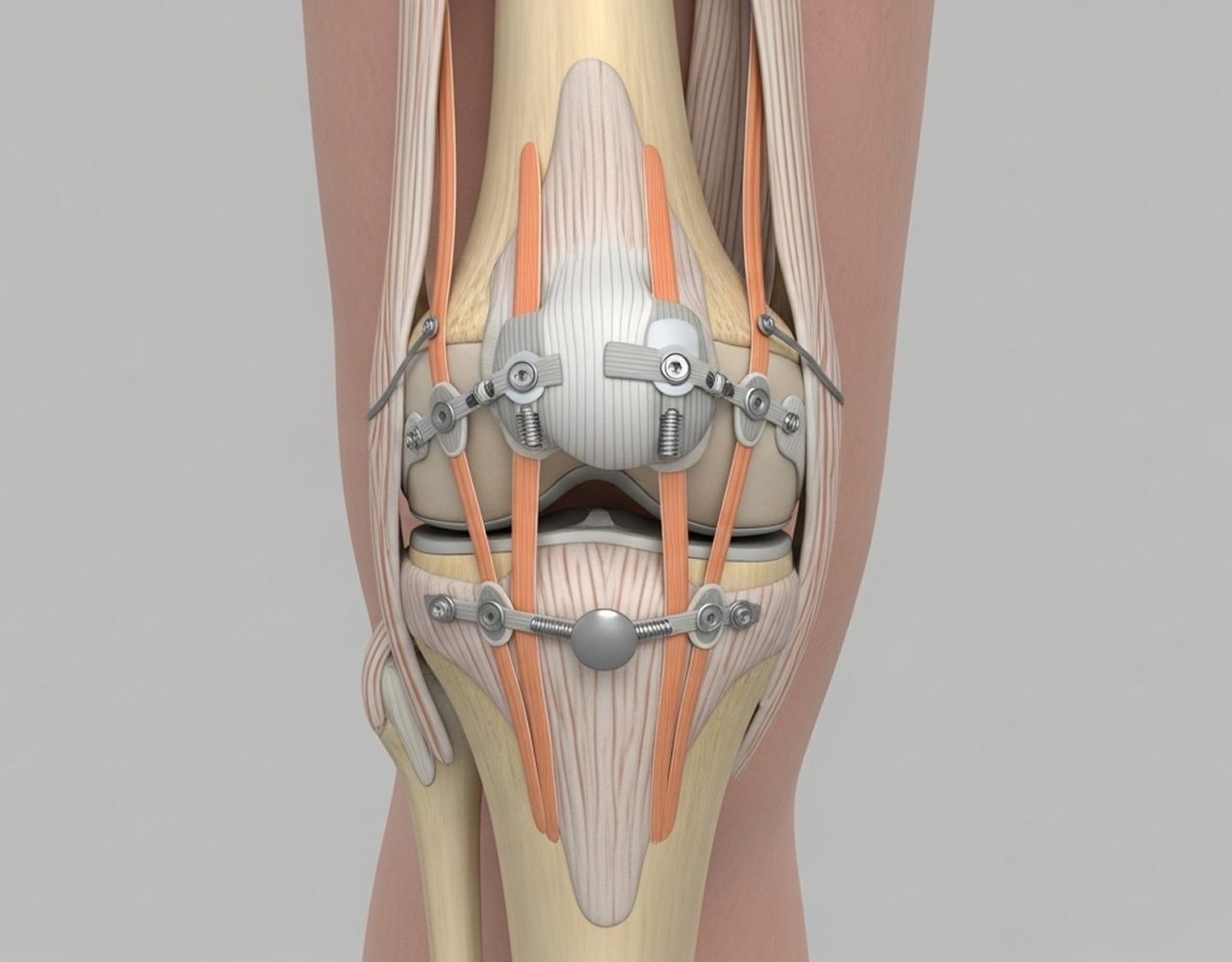
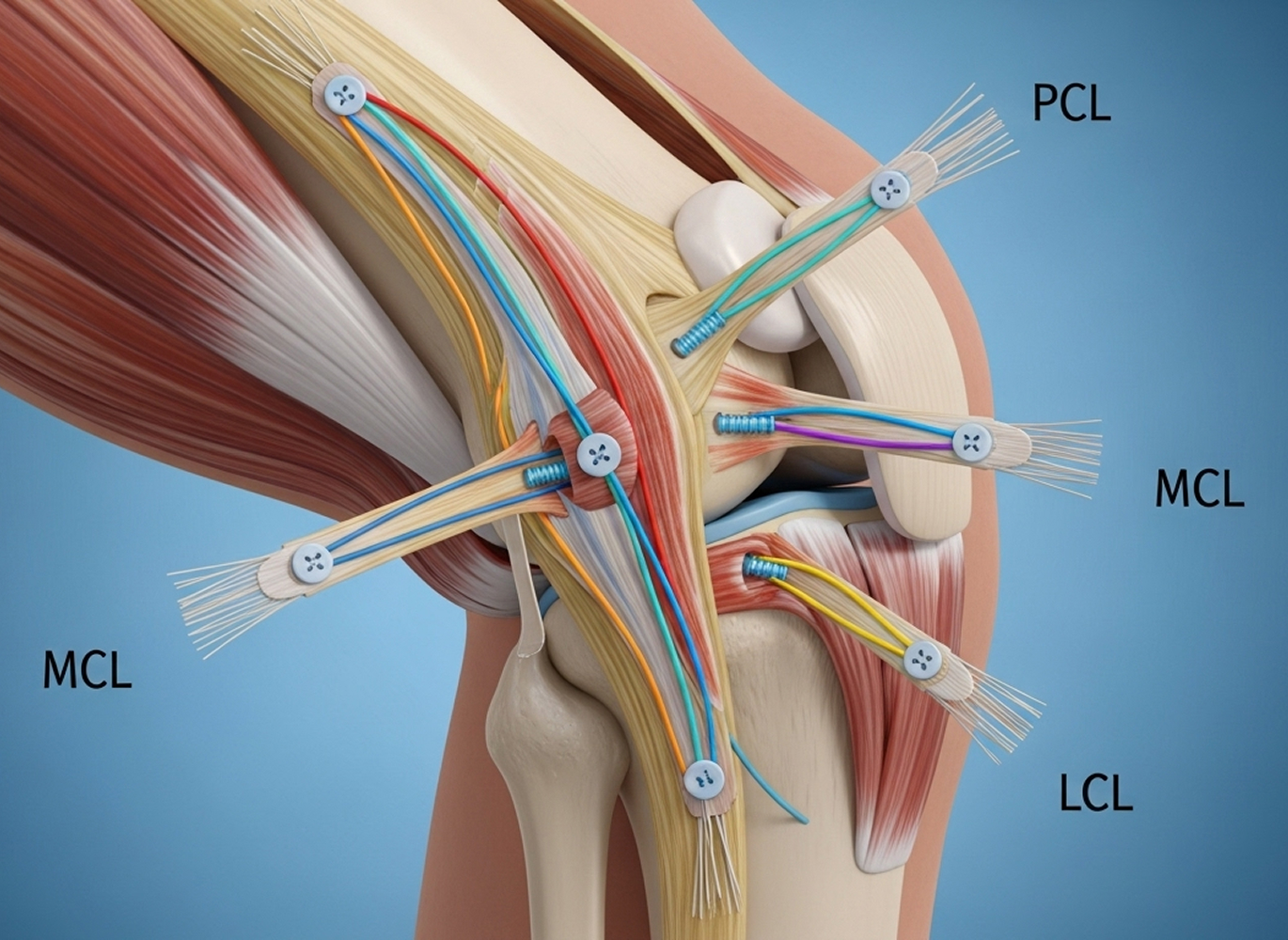
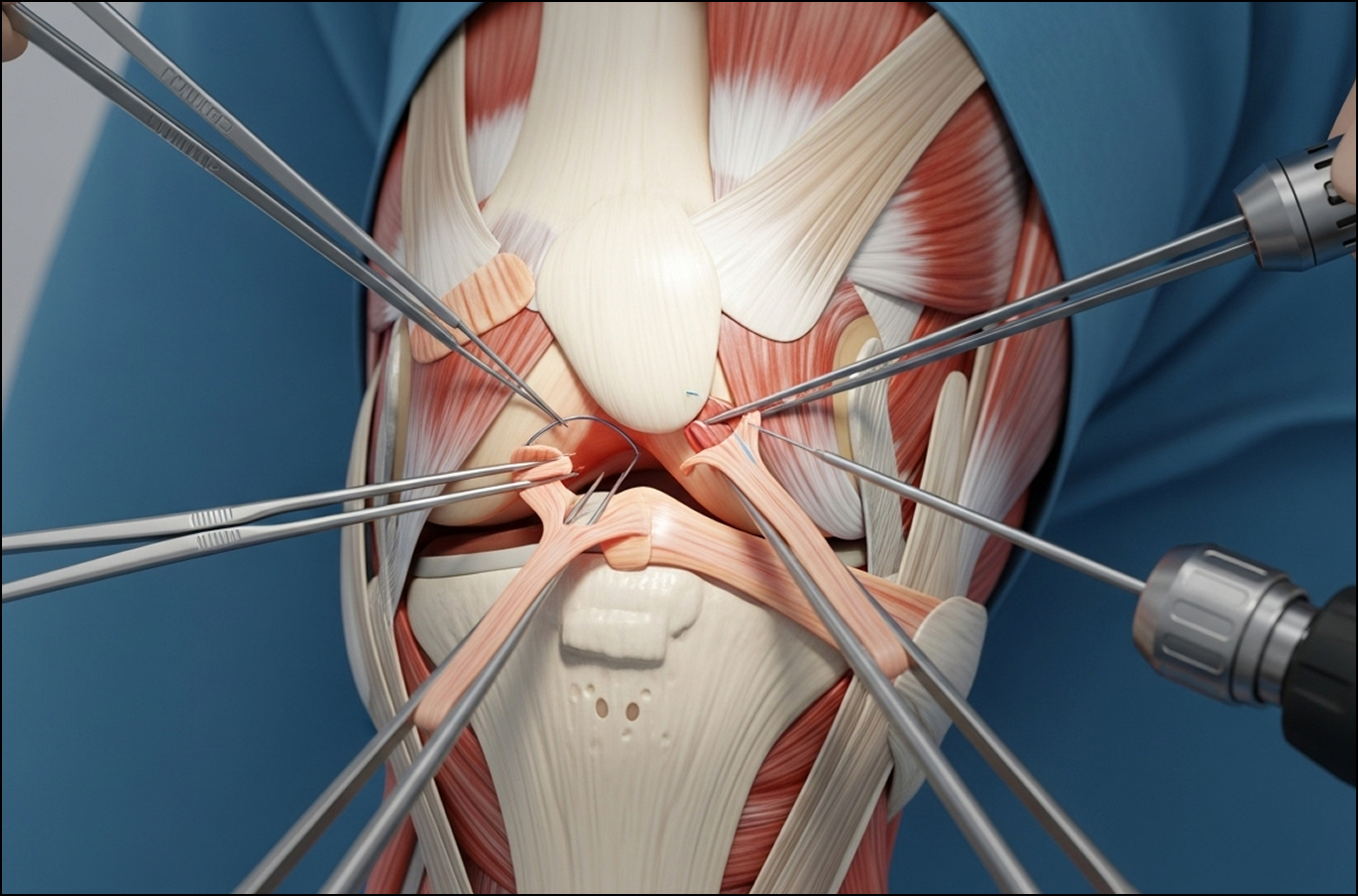
Multiligament reconstruction is a complex operation requiring meticulous planning and execution.
Dr Allom often uses a hybrid approach. This typically involves using your own hamstring tendon (autograft) for the primary cruciate ligament (like the ACL) and using donor tissue (allograft) for the other ligaments and corner structures. This balances graft strength with tissue availability.
Recovering from multiligament reconstruction is a marathon, not a sprint. It is significantly longer and more complex than recovery from an isolated ligament surgery and demands your full commitment.


Possesses dual UK and Australian qualifications (FRCS (Eng), FRACS (Orth) with specific fellowship training in complex knee reconstruction techniques, including ACL/PCL injuries and corner instability.
What to Bring: Please bring your referral letter, all relevant imaging studies (X-rays, CT scans, MRI if performed), and your list of current medications to your consultation.

