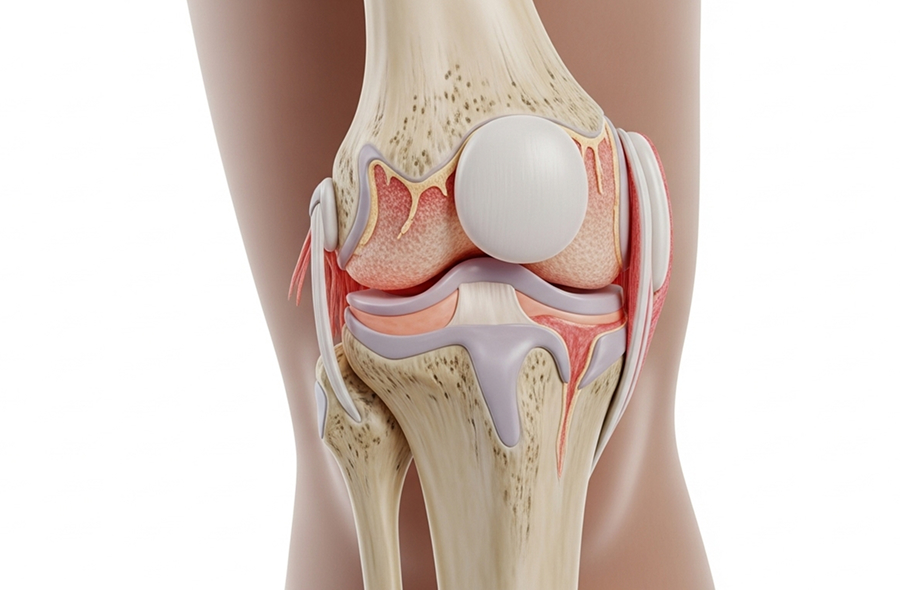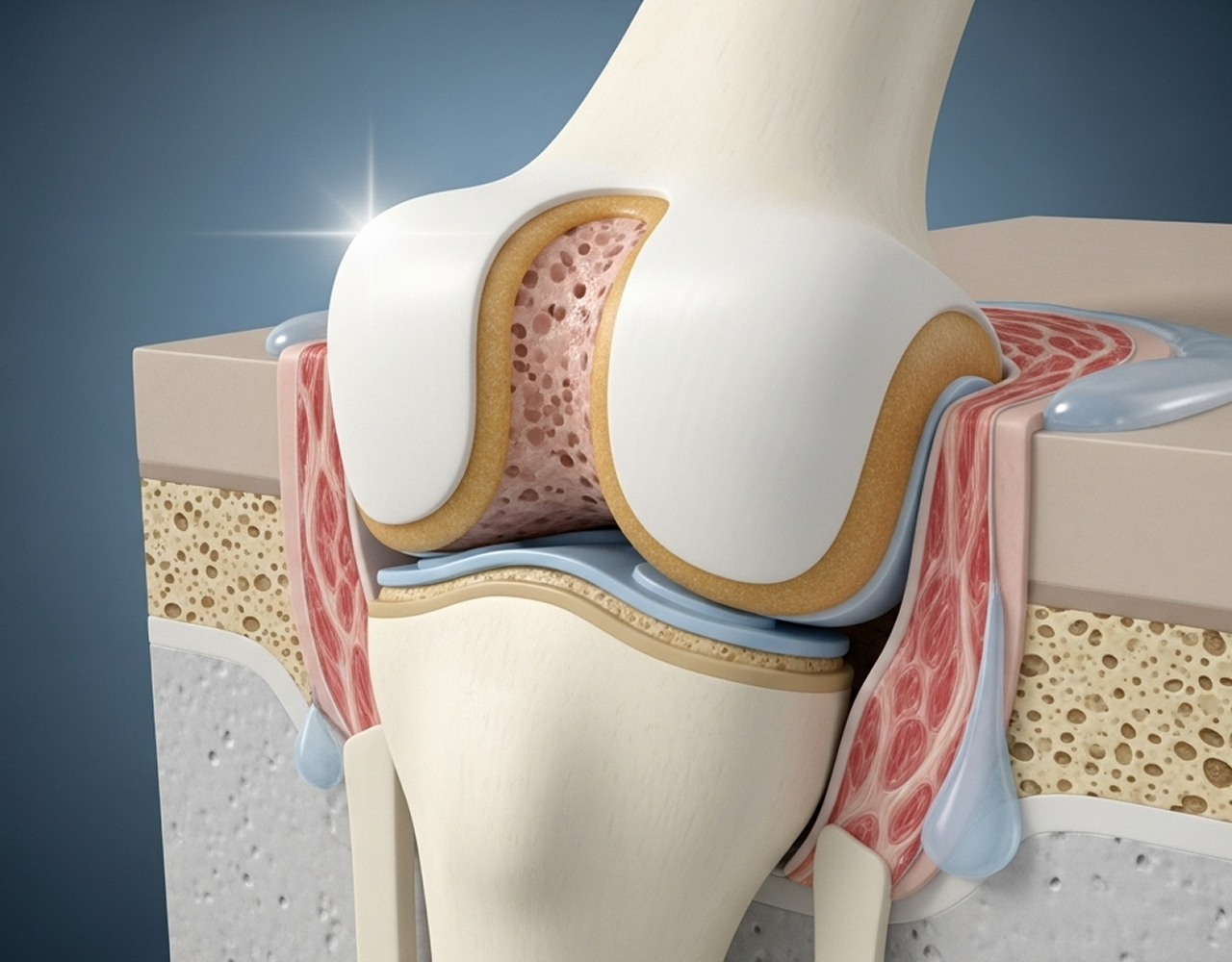
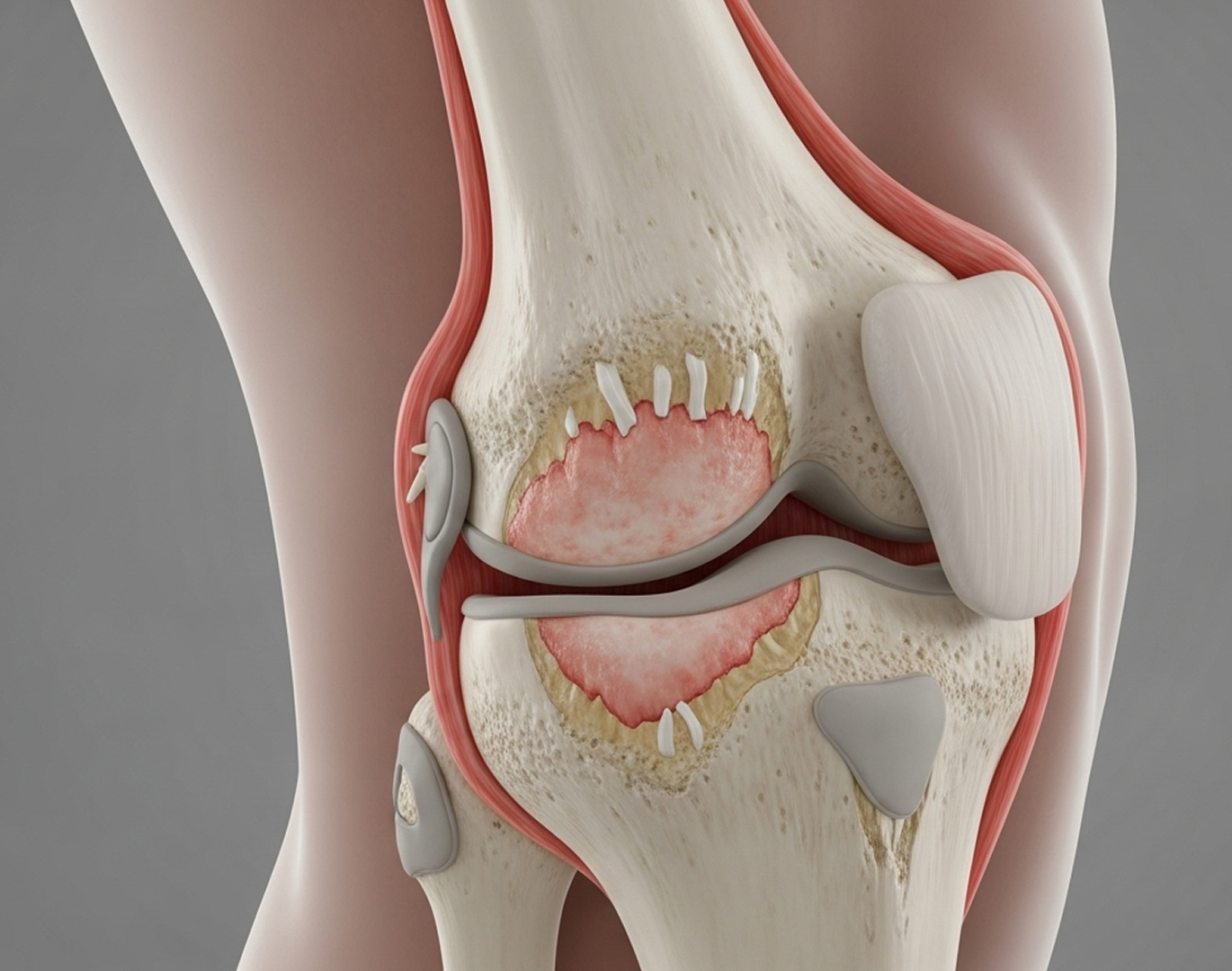
Patellofemoral arthritis affects the joint between your kneecap (patella) and the thighbone (femur). You might hear it called 'kneecap arthritis'. While the main knee joint often remains healthy, the smooth cartilage behind the kneecap can wear down. This typically causes pain when you climb stairs, squat down, or sit for long periods.
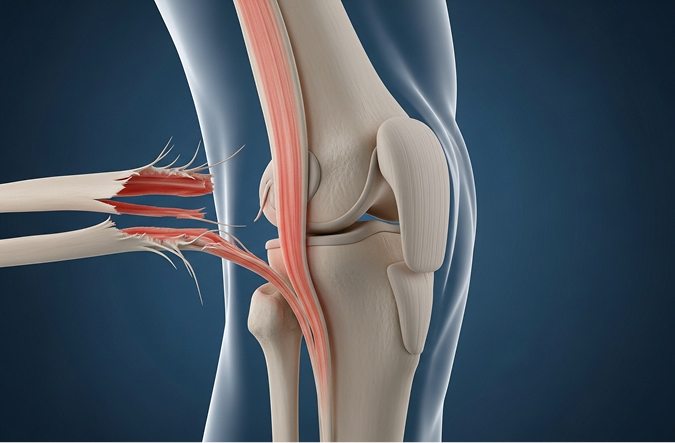
Think about the forces going through your kneecap joint. It handles two to three times your body weight just walking, and up to seven times when you squat or use stairs. Over time, repetitive stress, a previous injury, or if your kneecap doesn't track smoothly in its groove (malalignment) can lead to cartilage breakdown and arthritis.
This condition is quite common. Studies suggest 40-50% of people over 40 experiencing knee pain have some degree of patellofemoral arthritis. However, arthritis affecting only the kneecap joint (isolated patellofemoral arthritis) is less frequent, occurring in about 10-15% of knee arthritis cases.
If you suspect you have patellofemoral arthritis, or if pain behind your kneecap is affecting your daily activities and conservative treatments haven't provided enough relief, a specialist assessment is the next step. I welcome the opportunity to evaluate your knee, discuss your diagnosis, and explore the most appropriate treatment options for your individual situation.
What to Bring: Please bring your referral letter, all relevant imaging studies (X-rays, CT scans, MRI if performed), and your list of current medications to your consultation.
Source: British Journal of Sports Medicine - Patellofemoral Pain and Arthritis Management - 2024
If you are overweight, losing even a small amount of weight can make a big difference. Reducing body weight by 5-10 kg can significantly decrease stress on the kneecap joint, potentially cutting pain by 20-40%.
Surgery is considered only when comprehensive conservative management fails to provide adequate relief after 6-12 months, and your symptoms continue to significantly impact your quality of life. The right surgical option depends on your age, activity level, the severity and location of the cartilage damage, and your kneecap alignment.
This is a keyhole surgery procedure to smooth down roughened cartilage surfaces and remove any loose fragments within the joint. It's most effective for patients experiencing mechanical symptoms like catching or locking. While 60-70% of patients experience short-term improvement, the benefits often diminish over 1-2 years as the underlying arthritis progresses.
These techniques are typically reserved for younger patients (usually under 40) with specific, localised areas of cartilage damage, rather than widespread arthritis. Options include:
When used for appropriate, isolated defects, 70-80% of patients achieve good to excellent results at 5 years.
This procedure involves surgically repositioning the tibial tubercle. This is the bony bump on the shin bone where the patellar tendon attaches. Moving it can change the forces acting on the kneecap, offloading the damaged cartilage area and improving alignment. It's typically considered for younger, active patients with clear evidence of kneecap malalignment and associated cartilage damage.
This procedure replaces only the worn surfaces of the kneecap (patella) and the groove in the thighbone (trochlea) with artificial components, leaving the healthy main knee joint (tibiofemoral joint) intact.
Source: The Knee Journal - Patellofemoral Arthroplasty Outcomes - 2024
This involves replacing all three compartments of the knee joint (femur, tibia, and patella). It's reserved for patients who have significant arthritis affecting both the patellofemoral joint and the main tibiofemoral joint, or for cases where a previous patellofemoral replacement has failed. It is a larger operation with a typically longer recovery period compared to patellofemoral replacement.
My philosophy is always to exhaust appropriate non-surgical options first. Most patients can achieve meaningful improvement in their symptoms through a dedicated programme of physiotherapy, activity modification, weight optimisation if needed, and sometimes bracing or orthotics. Surgery is only considered when these measures fail to provide adequate relief and your quality of life remains significantly affected.


When surgery is the right choice, I offer the full spectrum of evidence-based patellofemoral procedures. This includes arthroscopic debridement, tibial tubercle osteotomy for realignment, patellofemoral joint replacement, and, when necessary, total knee replacement or revision surgery.
My recommendations are always tailored to your individual circumstances. Factors like your age, activity level, the exact pattern and severity of cartilage damage, your kneecap alignment, and your personal goals all play a part in deciding the best path forward. I am committed to providing honest, evidence-based advice specific to your situation, ensuring you can make an informed decision about your care.
Recovery times vary depending on the specific procedure performed.
Here's a general guide for Patellofemoral Joint Replacement:
Distinguishing isolated patellofemoral arthritis requires a specialist assessment. This includes a thorough clinical examination, specific weight-bearing X-rays (including a 'skyline' view of the kneecap), and usually an MRI scan to evaluate the cartilage in all three compartments of the knee (patellofemoral, medial tibiofemoral, lateral tibiofemoral). During your consultation, I will carefully assess whether your arthritis is truly confined to the kneecap joint, which is crucial for determining the most appropriate treatment options.
Arthritis itself, meaning the cartilage wear, does not spontaneously improve or reverse. However, the symptoms associated with it—pain, stiffness, and functional limitation—can often improve significantly with the right conservative treatments like physiotherapy, activity modification, and weight management. Many patients achieve long-term control of their symptoms without needing surgery.
It depends on where the arthritis is located. For patients with arthritis only affecting the kneecap joint (isolated patellofemoral arthritis), a patellofemoral joint replacement offers several potential advantages. It preserves the healthy main knee joint surfaces and ligaments, often leads to a faster recovery (typically 2-3 months compared to 4-6 months for a TKR), and may result in a more natural feeling knee. However, if you have significant arthritis in the main compartments of your knee as well, then a total knee replacement is usually the more appropriate and durable solution.
This is a known potential long-term outcome. Studies suggest that around 10-15% of patients may develop significant arthritis in the previously healthy tibiofemoral compartments over a 10-year period following patellofemoral replacement. If this happens and causes significant symptoms, the patellofemoral replacement can be successfully converted to a total knee replacement. This is a well-established revision procedure with generally good outcomes.
Most patients experience a significant reduction in their anterior (front of knee) pain after appropriately performed patellofemoral surgery. However, it's important to have realistic expectations. Around 10-15% of patients may still have some residual mild discomfort. Complete pain elimination cannot be guaranteed. Patellofemoral arthritis surgery, in general, can have less predictable outcomes for pain relief compared to standard total knee replacement for widespread arthritis.
Generally, a thorough trial of 6-12 months of comprehensive conservative management is recommended before considering surgery for patellofemoral arthritis. This should include a structured physiotherapy programme (minimum 12 weeks), consistent activity modification, weight optimisation if needed, and appropriate use of aids like bracing, orthotics, or medications. Surgery becomes a consideration when your symptoms remain significantly disruptive to your quality of life despite these dedicated non-operative efforts.
Chondromalacia patellae typically refers to softening or early fraying of the cartilage behind the kneecap, often seen in younger individuals, and frequently related to overuse or minor malalignment. It's often manageable with conservative treatment like physiotherapy.
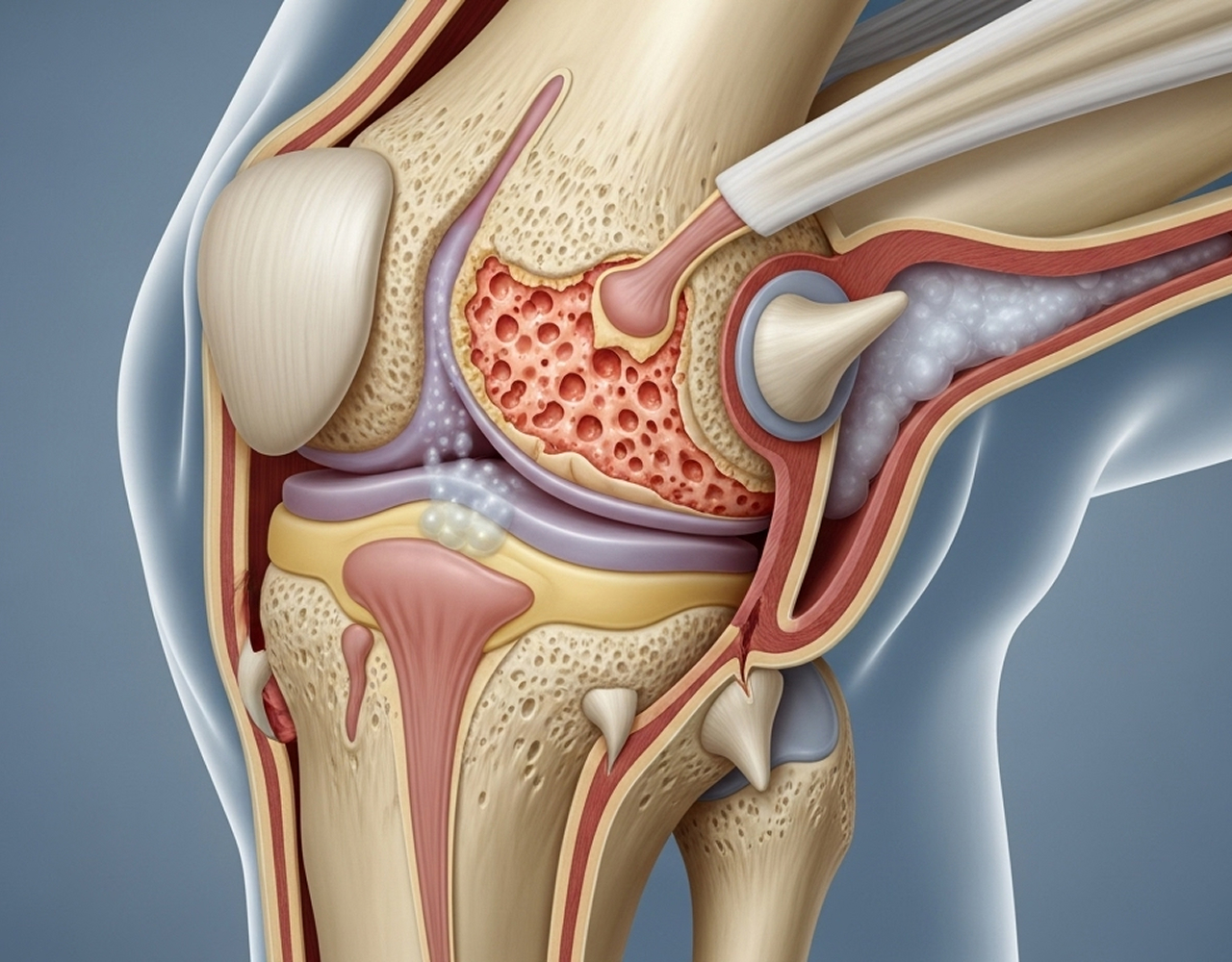
Patellofemoral arthritis represents more established degenerative change, involving significant cartilage loss, thinning, and potentially underlying bone changes like bone spurs (osteophytes). It's more common in older individuals (though can occur earlier) and may be less responsive to conservative measures alone.
Medical Disclaimer: The information provided on this page is for general educational purposes only and does not constitute professional medical advice. Diagnosis and treatment for patellofemoral arthritis should always be based on a thorough assessment by a qualified healthcare professional, including a clinical examination and review of appropriate imaging. Individual results may vary.
For Referring Doctors: I welcome referrals for patients with suspected isolated patellofemoral arthritis, particularly those who have failed conservative management or require specialist assessment for surgical options. Direct contact details for case discussion are available in the 'For Referring Doctors' section.