Tendon Repair Surgery for Patellar and Quadriceps Ruptures
A patellar or quadriceps tendon rupture is a serious knee injury needing prompt surgery to repair the tear and restore your ability to straighten the leg. Dr Richard Allom is a fellowship-trained knee subspecialist providing expert surgical repair for these injuries across South West Sydney and the Mid North Coast.
Urgent Surgery is Key
Repair within 2-3 weeks offers the best chance for full recovery.
Expert Repair
Dr Allom uses advanced techniques to securely stitch the tendon back together, promoting effective healing.
Restored Function
Successful surgery followed by dedicated rehabilitation helps most patients return to their previous activities.
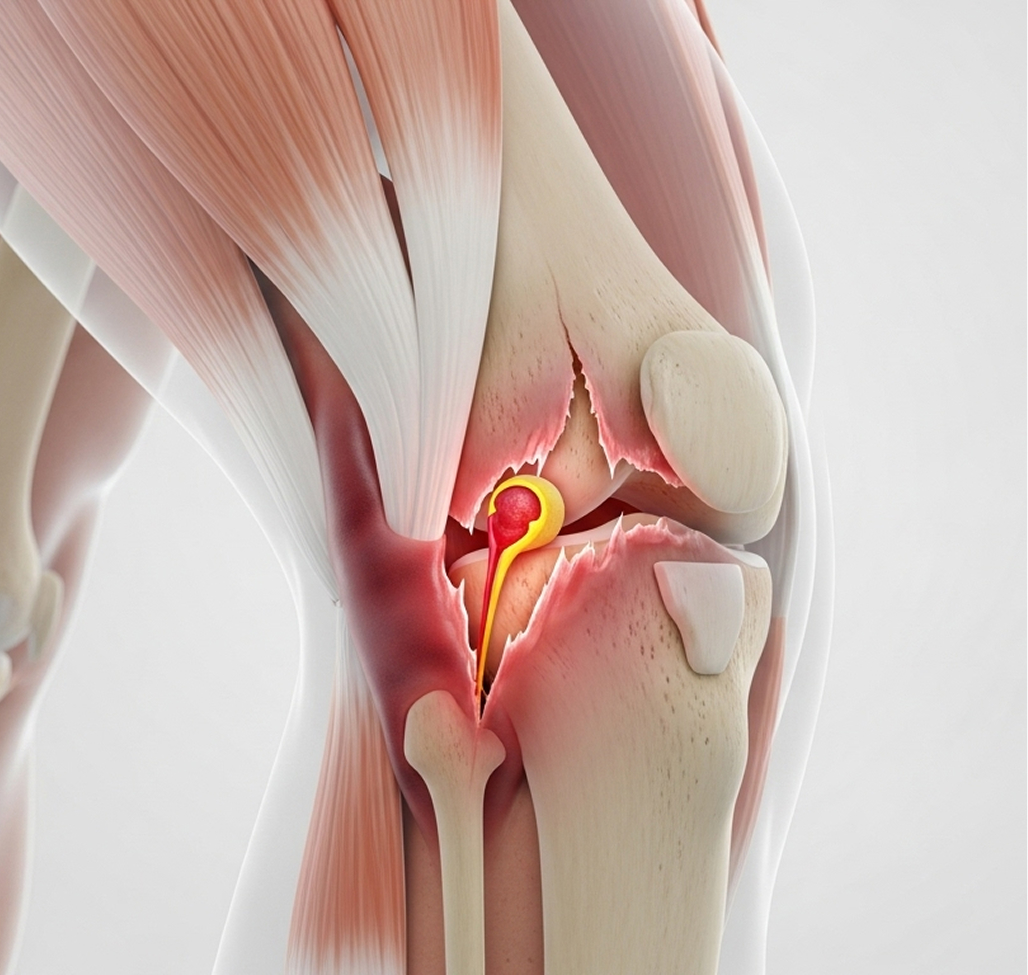
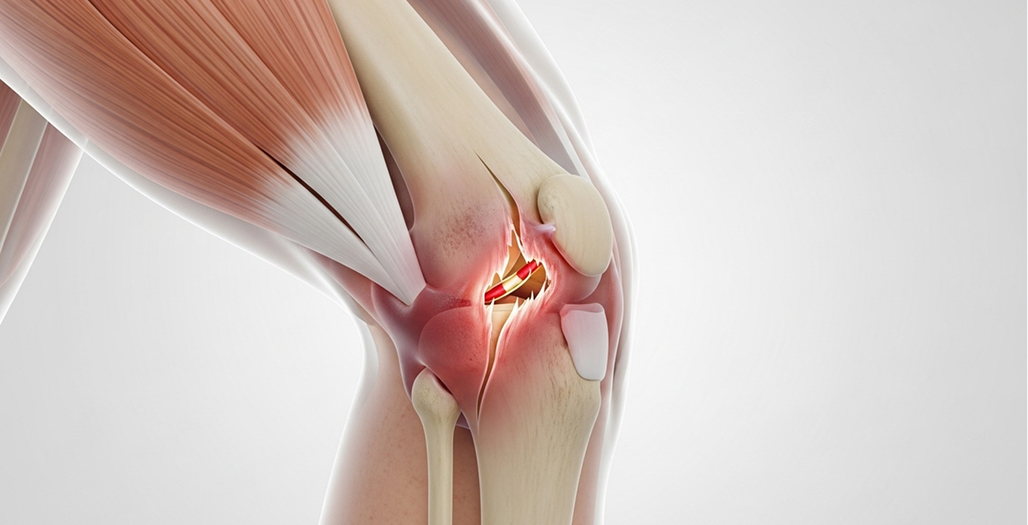
Understanding Knee Tendon Ruptures
A sudden tear, or rupture, in your patellar or quadriceps tendon is a significant injury. These tendons are crucial parts of your knee's extensor mechanism. This is the system connecting your thigh muscles to your shin bone, allowing you to straighten your knee. When one of these tendons tears completely, you lose the ability to actively straighten your leg, making walking, standing, or climbing stairs extremely difficult or impossible.
If you have ruptured one of these tendons, you likely felt a tearing sensation or 'pop' and now experience:
Severe pain and swelling at the front of your knee.
Inability to straighten your knee against gravity.
A noticeable gap where the tendon has torn.
Difficulty standing or walking as the knee may buckle.
The positive news is that prompt surgical repair is highly effective. It can restore knee function for most people, allowing a return to daily activities and even sports.
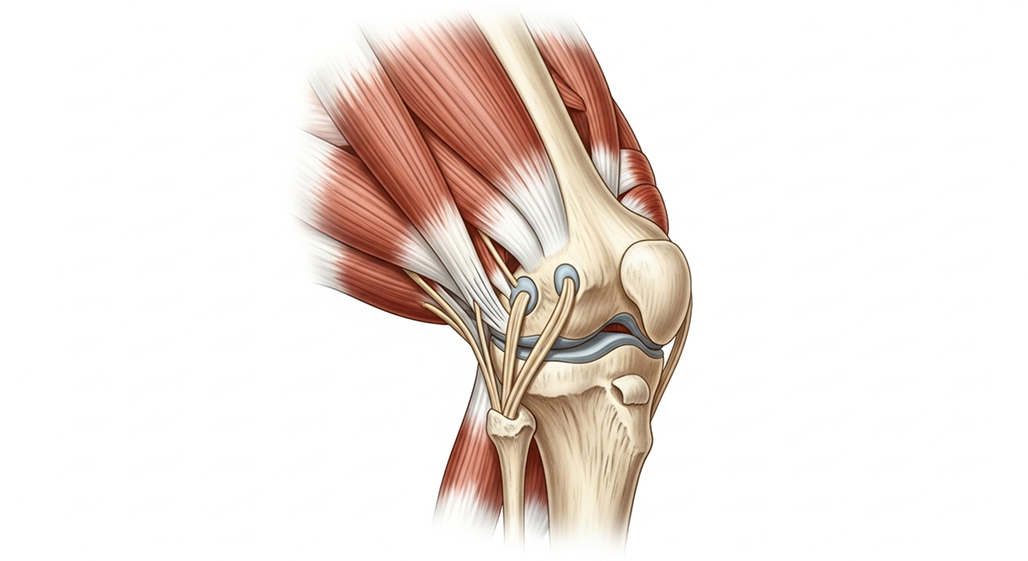
Your Knee's Extensor Mechanism
Think of straightening your knee like pulling a rope over a pulley. Your powerful quadriceps muscles in the thigh provide the pull. This force travels through the quadriceps tendon, over the patella (kneecap, the pulley), down through the patellar tendon, and attaches to the top of your shin bone (tibia). A tear in either the quadriceps or patellar tendon breaks this chain, disrupting the power needed to straighten the leg.
How Do These Tendon Ruptures Happen?
These tears often occur due to sudden, forceful events, although underlying factors can weaken the tendon over time.
Patellar Tendon Rupture
Common Causes
Often happens during sports involving jumping or sudden changes in direction, like landing awkwardly from a jump or a rapid deceleration. Forceful extension against resistance, like in weightlifting, can also cause it.
Who is Affected
Typically affects active individuals aged 30-40, particularly males involved in sports like basketball, rugby, or football.
Quadriceps Tendon Rupture
Common Causes
Can result from similar forceful events but often occurs with less force in older individuals, sometimes during simple activities like stumbling or missing a step.
Who is Affected
More common in people aged 50-60+, often associated with pre-existing tendon weakness or degeneration.
Factors Increasing Rupture Risk
Certain conditions and factors can make tendons weaker and more prone to tearing:
Medical Conditions
Chronic kidney disease, diabetes, rheumatoid arthritis, gout, and lupus can affect tendon health.
Medications
Long-term use of corticosteroids (oral or multiple injections) or certain antibiotics (fluoroquinolones) can weaken tendons. Anabolic steroid use is also a risk factor.
Previous Injury
Prior knee surgery (like ACL reconstruction using a patellar tendon graft), or chronic tendon inflammation ('jumper's knee') can increase risk.
Recognising the Symptoms and Getting Diagnosed
Recognising a tendon rupture quickly is vital for getting timely treatment.
Immediate Signs
Most people feel or hear a 'pop' or tearing sensation at the moment of injury, followed immediately by:
Severe pain at the front of the knee.
Inability to straighten the leg or stand on it.
Rapid swelling and bruising.
Sometimes, a visible gap or defect can be felt in the tendon area.
The kneecap might look out of place. It might be sitting too high (patellar rupture) or too low (quadriceps rupture).
Diagnosis with Dr Allom
Dr Allom will perform a thorough clinical examination, looking for key signs:
Visual Check
Assessing swelling, bruising, and kneecap position.
Palpation
Gently feeling for a gap in the tendon.
Straight Leg Raise Test
Asking you to lift your straight leg while lying down. Inability to do this is a classic sign of a complete rupture.
Extension Lag Check
Measuring the difference between how far you can straighten the knee passively (with help) versus actively (on your own).
Imaging Tests
Imaging confirms the diagnosis and helps plan surgery:
X-rays
Essential to check kneecap position and rule out fractures. They can sometimes show if a piece of bone has been pulled off with the tendon.
Ultrasound
Can directly visualise the tear, its size, and any associated fluid collection.
MRI Scan
Provides the most detailed view, showing the exact location and extent of the tear, tendon quality, and any other associated knee injuries.
Remember: Early diagnosis is crucial. Seeking prompt assessment leads to better repair options and outcomes.
Is Surgical Repair Necessary?
For most patellar and quadriceps tendon ruptures, surgery is the recommended treatment.
When Surgery is Essential
Complete Tears
If the tendon is completely torn, surgery is almost always required. The separated ends will not heal back together on their own. Surgery brings the torn ends together, allowing them to heal properly.
Partial Tears with Significant Weakness
Even some partial tears need surgery if they cause major weakness in straightening the knee or significantly limit your function. Repair can prevent the tear from becoming complete and restore full strength
Active Individuals
Anyone needing strong knee extension for work, sports, or an active lifestyle typically requires surgery to regain full function.
Why Timing Matters The Urgency for Repair
Surgery performed soon after the injury generally leads to better results.
Acute Repair
Within 2-3 weeks
This is the ideal timeframe. The tendon tissue is healthier, there's less scarring, and a direct repair is usually possible. Recovery is typically faster with better functional outcomes.
Delayed Repair
After 3 weeks
The tendon starts to retract (pull back) and scar tissue forms, making the repair more challenging. Muscle wasting (atrophy) also begins. More complex surgical techniques, possibly involving grafts, might be needed.
Chronic Cases
Months later
Repair becomes very difficult due to significant tendon retraction, scarring, and muscle deterioration. Reconstruction using tissue grafts (allograft) or synthetic materials may be necessary, and outcomes are often less predictable.
The key message: Aim for surgical repair within the first few weeks for the best possible outcome.
When Surgery Might Not Be Advised
In rare cases, surgery might be too risky, such as in individuals with severe medical problems, active infections, or very poor skin condition around the knee. For very sedentary, elderly individuals with low functional demands, non-surgical management with bracing might be considered after careful discussion, but this is uncommon for complete tears.
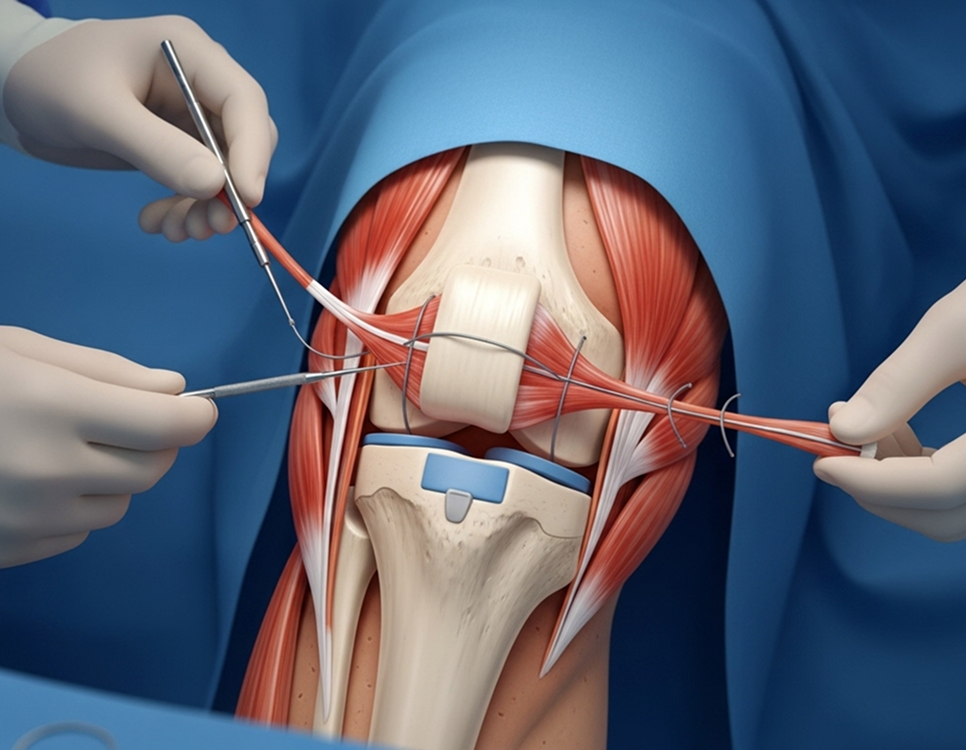
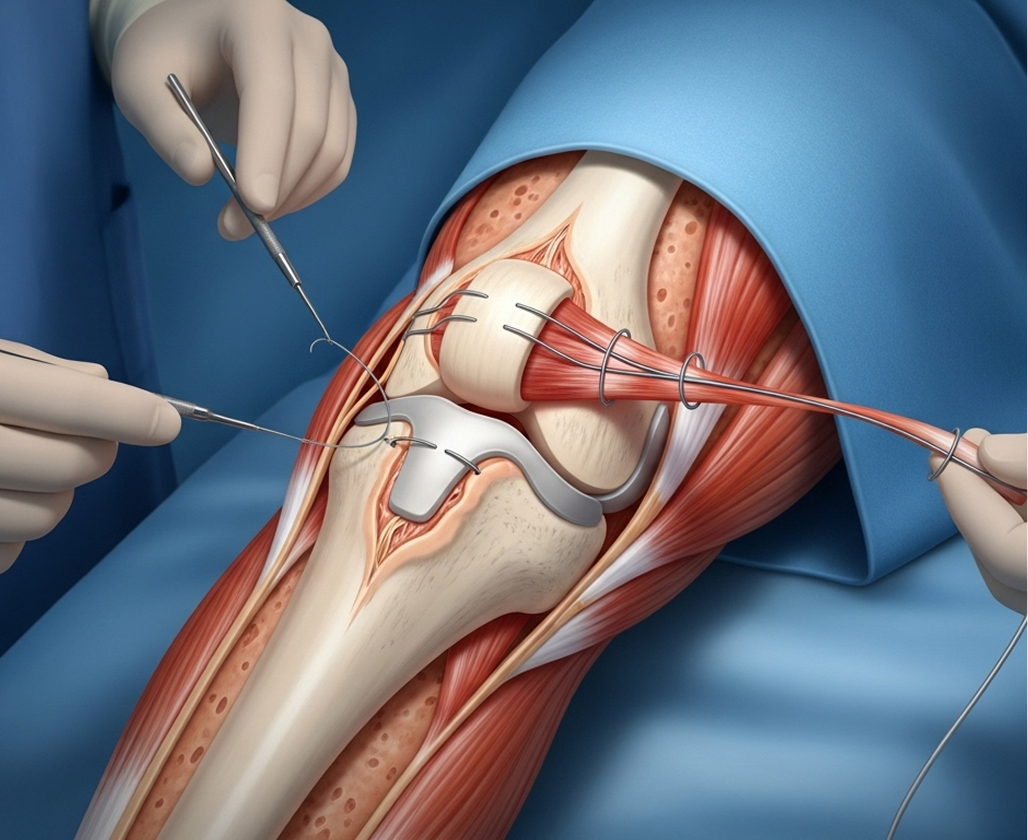
Tendon Repair Surgical Techniques
Dr Allom employs proven surgical methods tailored to your specific injury. The goal is a strong, secure repair that allows for effective rehabilitation.
Primary Tendon Repair
This is the standard approach for acute ruptures.
Preparation
A midline incision is made over the front of the knee. Any blood clot is cleared, and the torn tendon ends are prepared for stitching.
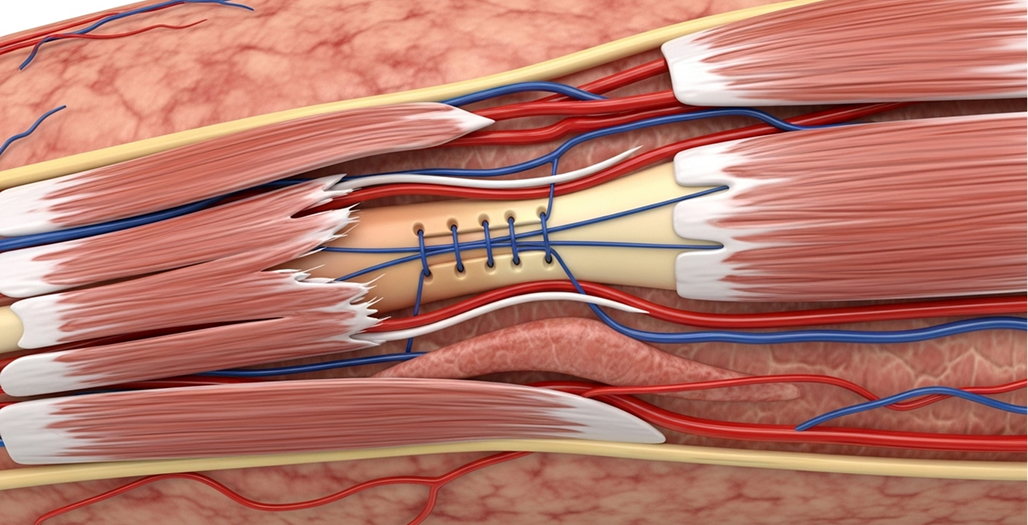
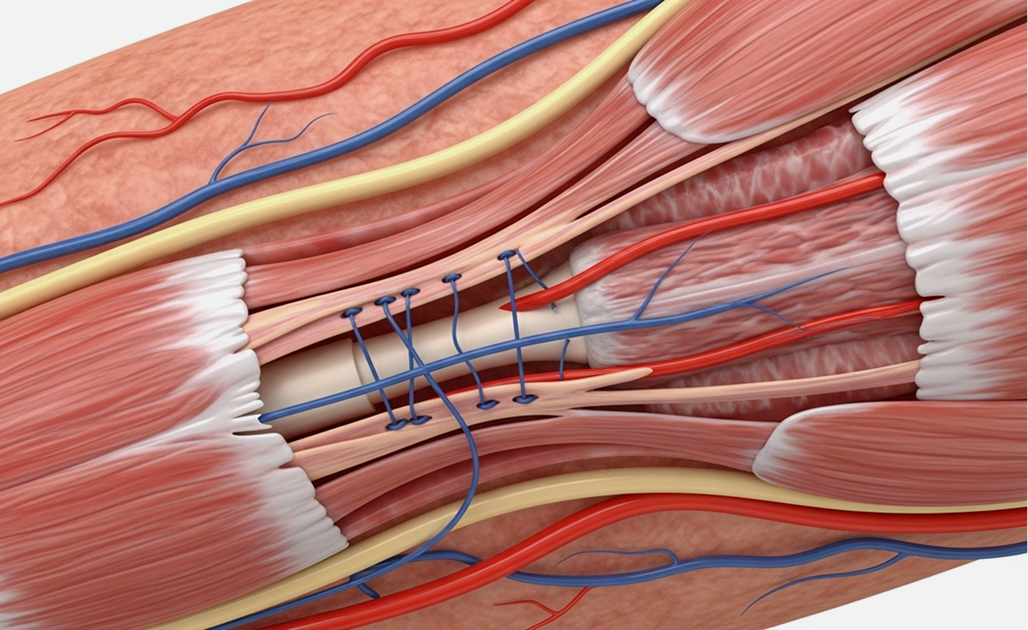
Suture Technique
Dr Allom typically uses strong, braided sutures woven through the tendon ends in a locking pattern (like the Krackow technique).
Fixation
The sutures are then securely fixed to the bone (either the kneecap or the shin bone) using tunnels drilled through the bone or specialised bone anchors.
Augmentation (if needed)
In cases of poorer tendon quality, delayed repairs, or revisions, the repair might be reinforced with additional sutures, wires, or synthetic materials for extra strength.
What to Expect on Surgery Day
Anaesthesia
Usually performed under general or spinal anaesthesia.
Duration
The surgery typically takes 60 to 90 minutes.
Hospital Stay
Most patients stay 1 or 2 nights in hospital.
Immediately After
Your knee will be placed in a brace locked straight (in extension), and you will use crutches for support, usually bearing weight as tolerated.
Recovery and Rehabilitation After Tendon Repair
Recovering from tendon repair takes time and dedication. The rehabilitation programme carefully balances protecting the healing tendon with gradually restoring movement and strength. Adhering strictly to the protocol, especially in the early stages, is vital for success.
Phase 1: Protection and Early Healing
Weeks 0-6
This is the most critical phase for protecting the repair.
Brace: You will wear a knee brace locked straight for walking initially. It will be gradually unlocked for controlled bending exercises as guided by Dr Allom and your physiotherapist.
Weight-Bearing: Usually allowed to put weight on the leg as comfortable, using crutches for balance and support.
Movement: Gentle, controlled knee bending exercises begin early, increasing gradually week by week (e.g., 0-30 degrees weeks 0-2, progressing towards 90 degrees by week 6).
Exercises: Focus on ankle pumps, gentle quad activation, and straight leg raises (only when cleared by physio).
Phase 2: Restoring Motion and Strength
Weeks 6-12
Once the initial healing is sufficient, the focus shifts to regaining movement and building strength.
Brace: Usually discontinued around week 6.
Movement: Aim to achieve full bending and straightening of the knee.
Exercises: Progressive strengthening begins. Examples include mini-squats, leg presses, step-ups, and stationary cycling (once sufficient bend is achieved).
Gait: Focus on normalising your walking pattern without crutches.
Phase 3: Building Functional Strength
Months 3-6
Strength and control become the main goals.
Strength Target: Aim for quadriceps strength to reach around 80% of your uninjured side.
Exercises: More advanced resistance training, balance exercises, and potentially starting low-impact activities like swimming or cycling.
Neuromuscular Control: Exercises to improve coordination and joint position sense.
Phase 4: Returning to Activities
Months 6-12+
The final phase involves gradual return to higher-level activities and sports.
Readiness Criteria: Before returning to demanding activities or sports, you need to meet specific criteria, including near-equal strength compared to the uninjured leg (≥90%), full range of motion, no pain, and successful completion of functional tests.
Timeline: Return to recreational activities often occurs around 6-9 months. Return to competitive or high-impact sports usually takes 9-12 months, sometimes longer for elite athletes.
Dr Allom works closely with your physiotherapist, providing a detailed protocol to guide your rehabilitation journey safely and effectively.
Expected Outcomes After Tendon Repair
Surgical repair generally leads to good outcomes, especially when performed early.
Success Rates
Acute repairs (within 2-3 weeks) typically result in good to excellent outcomes in 85-95% of cases. Delayed repairs have lower success rates, around 65-80%.
Functional Recovery
Quadriceps strength gradually returns over 12 months, often reaching 85-95% of the uninjured side. Most people return to daily activities within 3-4 months.
Return to Activity
Approximately 70-85% of patients can return to their previous level of activity or sport after an acute repair and dedicated rehabilitation.
Factors Influencing Outcomes
The best results are seen with early surgery, younger patients, good tendon quality, no significant medical problems, non-smokers, and importantly, excellent commitment to the rehabilitation plan.
Managing Risks and Complications
While tendon repair is generally safe and successful, potential complications can occur.
Possible Complications
Extension Lag
Some difficulty fully straightening the knee actively. Usually improves with physiotherapy but may require further intervention if severe.
Knee Stiffness
Reduced ability to bend the knee. Early physiotherapy helps prevent this.
Quadriceps Weakness
Common after surgery. Requires dedicated strengthening exercises for up to 18-24 months.
Re-rupture
This is reported in 2-5% of acute repairs, usually within the first 3 months if restrictions are not followed. Strict adherence to the post-operative protocol is the best prevention.
General Surgical Risks
Include infection (1-2%), blood clots (DVT/PE), wound healing issues, nerve numbness around the incision, or rarely, fracture.
Minimising Risks
Dr Allom takes several steps to minimise risks, including careful surgical technique, infection prevention protocols, blood clot prevention measures, and clear post-operative instructions. Your active participation in following restrictions and attending physiotherapy is also crucial.
Why Choose Dr Richard Allom for Your Tendon Repair
Choosing a surgeon with specific expertise in complex knee injuries is important for tendon repair surgery.
Fellowship-Trained Subspecialist
Dr Allom holds dual fellowships from the Royal College of Surgeons of England (FRCS) and the Royal Australasian College of Surgeons (FRACS). He has completed advanced fellowship training specifically focused on complex knee surgery, including tendon reconstruction.
Exclusive Knee Focus
His practice is dedicated solely to knee conditions, providing a depth of experience in managing acute and chronic tendon ruptures.
Advanced Techniques
Dr Allom utilises evidence-based surgical techniques, including high-strength suture methods and augmentation strategies when needed, combined with structured rehabilitation protocols designed for optimal recovery.
Accessible Care
He offers consultations and surgery across both South West Sydney (Gledswood Hills, Campbelltown, Liverpool) and the Mid North Coast (Taree, Forster), providing convenient access to subspecialist care.
Frequently Asked Questions
Most patients walk without aids and with a relatively normal gait by 6-8 weeks after surgery, once the brace is removed and initial strength returns. Minor adjustments in walking pattern may continue improving for 3-4 months.
No, a complete tear of the patellar or quadriceps tendon cannot heal properly without surgery. The torn ends pull apart (retract) and cannot bridge the gap naturally. Surgery is needed to bring the ends together and allow healing.
The patellar tendon connects the bottom of the kneecap to the shin bone, while the quadriceps tendon connects the thigh muscles to the top of the kneecap. Patellar ruptures are more common in younger athletes (30-40s), often causing the kneecap to sit too high. Quadriceps ruptures are more frequent in older individuals (50-60s) and cause the kneecap to sit too low. Both require similar urgent surgical repair.
With successful surgery and dedicated rehabilitation, most people can return to recreational sports (around 6-9 months) and competitive sports (around 9-12 months). Around 70-85% return to their previous level of activity.
Delaying surgery beyond the first 2-3 weeks makes the repair more difficult due to tendon retraction and scarring. More complex reconstruction techniques may be needed, and success rates are generally lower than for acute repairs.
Re-rupture is uncommon after an acute repair, occurring in about 2-5% of cases. The risk is highest in the first 6-12 weeks. Following the post-operative restrictions and physiotherapy protocol carefully significantly minimises this risk.
The key sign is the inability to actively straighten your knee against gravity after an injury. Other signs include a tearing sensation or 'pop', immediate severe pain, swelling, and often a palpable gap in the tendon or an abnormal kneecap position. If you suspect a rupture, seek urgent medical assessment.
Next Steps
If you suspect you have ruptured your patellar or quadriceps tendon, seeking specialist assessment quickly is vital. Prompt surgical repair within 2-3 weeks offers the best chance for a successful recovery.
What to Bring: Please bring your referral letter, all relevant imaging studies (X-rays, CT scans, MRI if performed), and your list of current medications to your consultation.