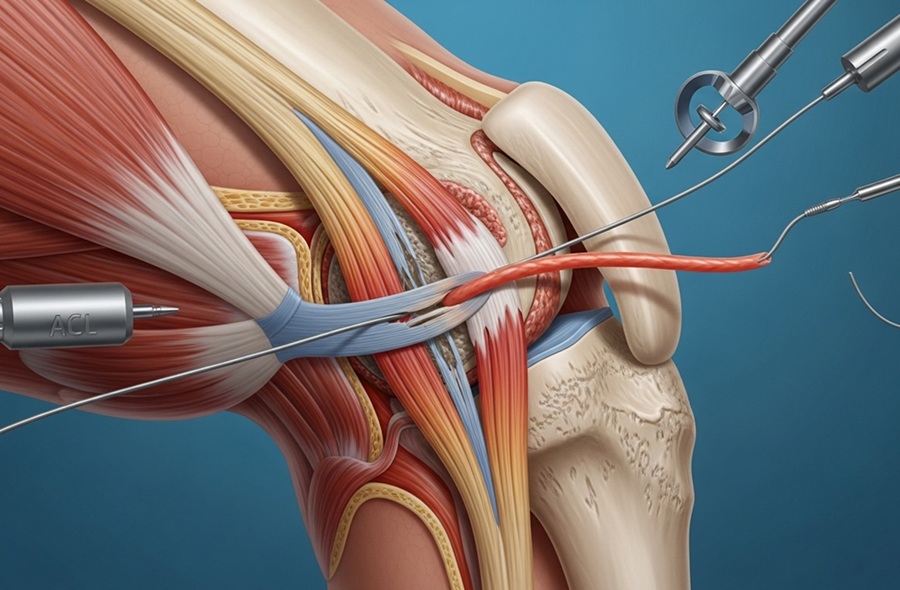

As a fellowship-trained knee subspecialist, Dr Allom provides complete ACL injury management, from initial diagnosis through to surgical reconstruction and rehabilitation. His subspecialist training means he is skilled in the latest arthroscopic techniques. His expertise is further supported by a Master's Degree in Surgery. He is dedicated to creating an individualised treatment plan based on your age, activity level, and personal goals. He takes the time to clearly explain your diagnosis and options so you can feel confident about your care.
"Look, I'm not here to push you toward surgery if you don't need it. Some of my patients do brilliantly without reconstruction. They modify activities, commit to rehab, and they're fine. But if you're 28 and you play competitive netball? We need to have a serious conversation about surgery, because without it, your knee will keep giving way and you'll likely tear your meniscus within a few years. I base my recommendation on what you want your life to look like. This depends on your age, your sport, your work demands, and what other injuries we find on your MRI. There's no one-size-fits-all answer here."
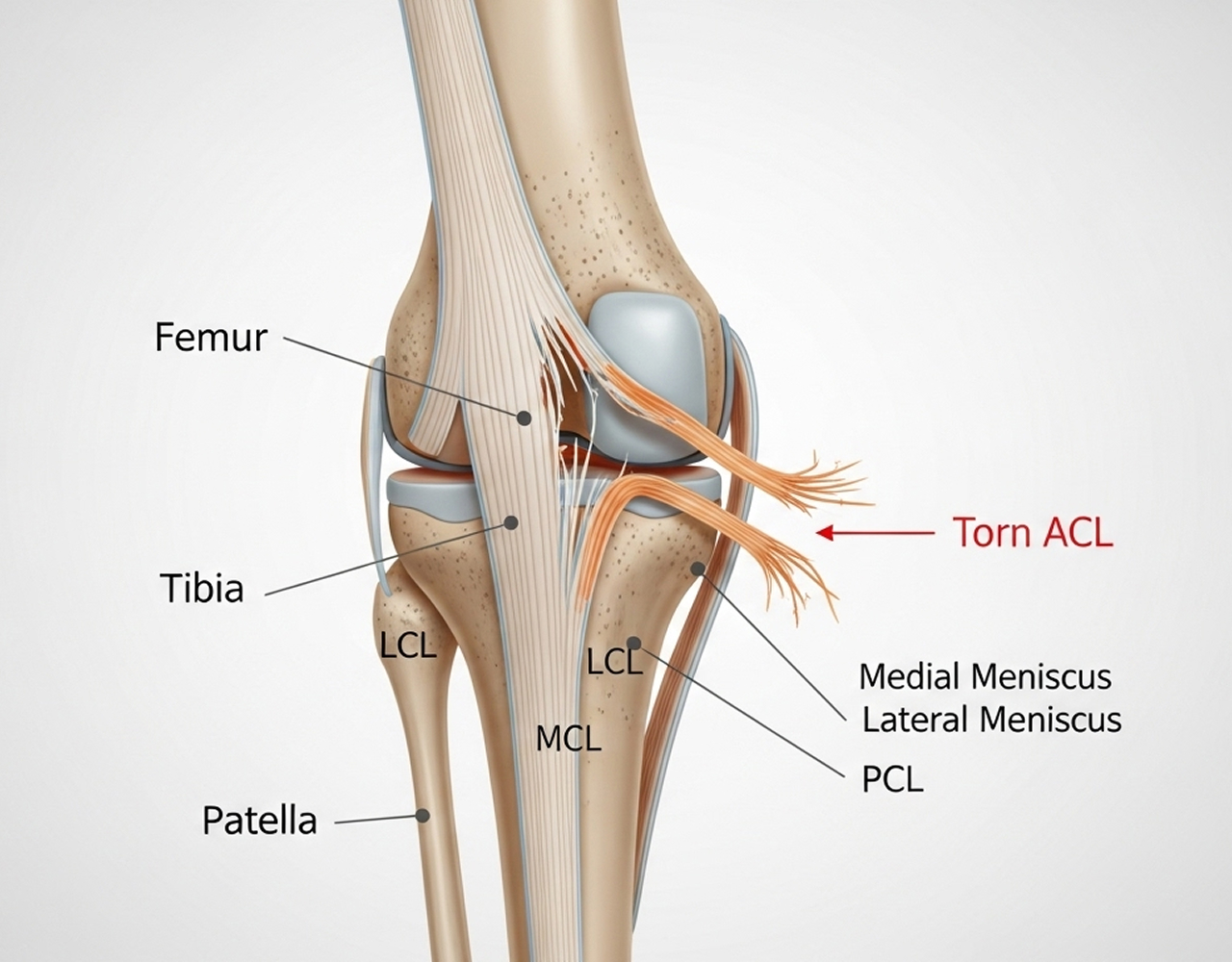
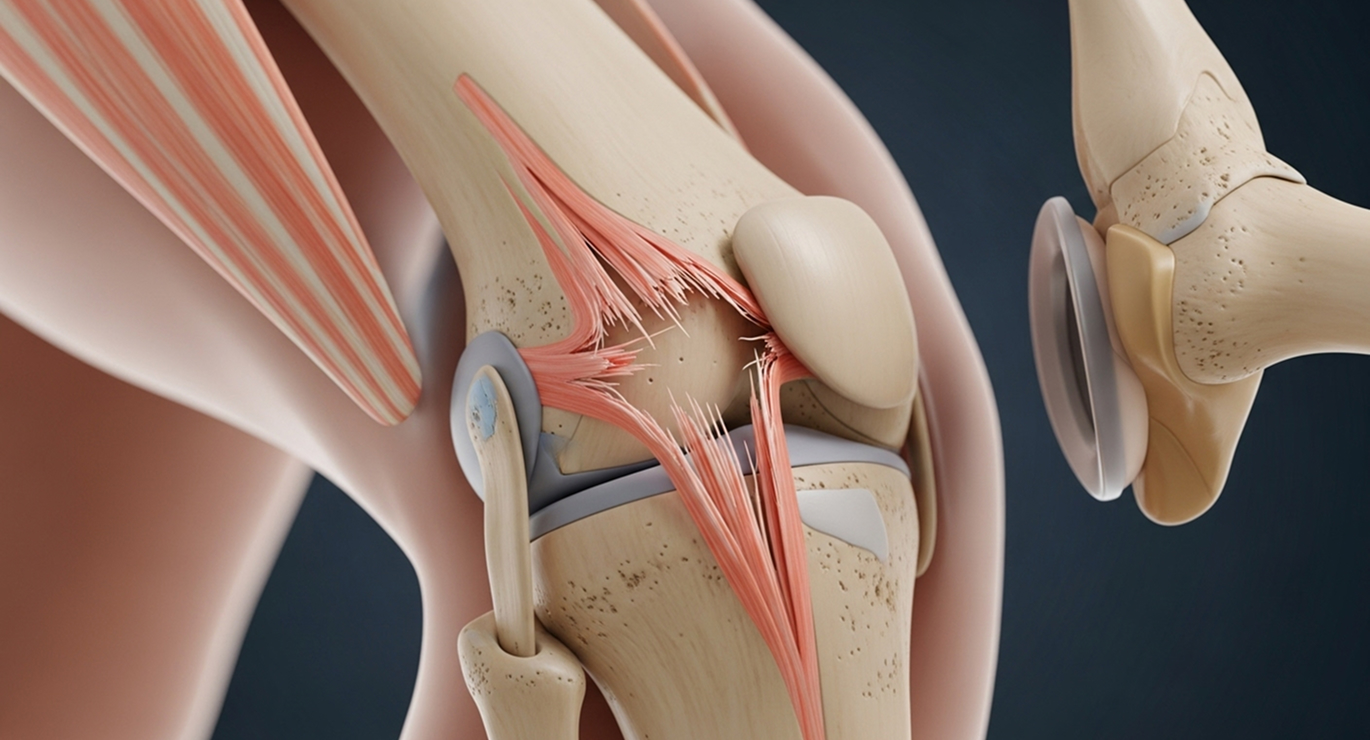
Unlike some other ligaments, the ACL has a very poor blood supply and does not heal on its own once it has a complete tear. Conservative management involves learning to function with the torn ligament, not waiting for it to heal.
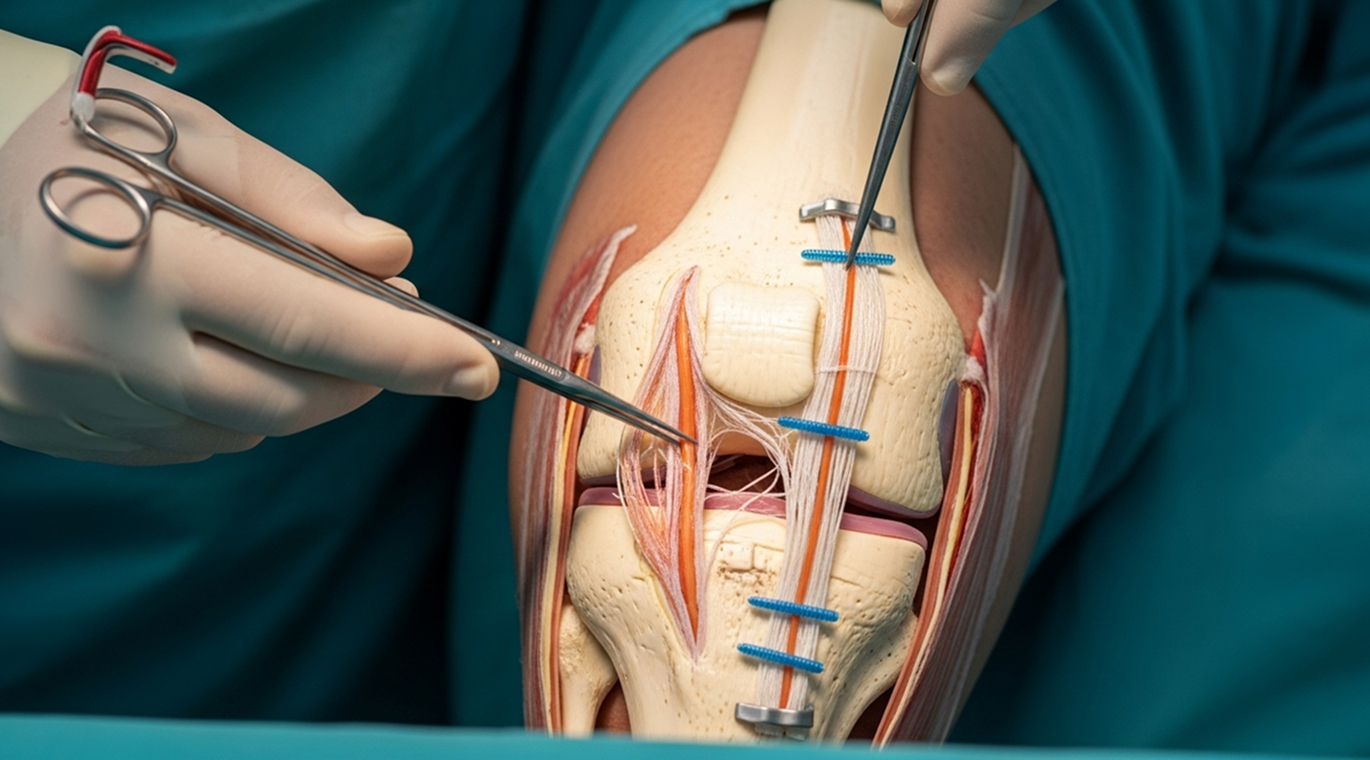
You will likely benefit from surgery if you want to return to sports that involve pivoting, cutting, or sudden stops (like football, netball, or skiing). It is also recommended if you experience recurrent instability during your daily activities, or if you have other associated injuries like a meniscal tear that needs repair.
For active individuals, untreated ACL deficiency carries significant risks. These include recurrent instability (giving way), a high risk of secondary meniscal tears (up to 40-50% within 5 years), and a much higher risk of developing early-onset osteoarthritis.
You can often delay ACL reconstruction for several weeks or even a few months without a negative impact. This allows time for the initial swelling to settle, for you to regain your full range of motion, and to properly consider your options. However, prolonged delays (over 6-12 months) while experiencing ongoing instability can increase your risk of secondary cartilage and meniscal damage.
After tearing one ACL, you have a 10-15% risk of tearing the ACL in your opposite knee. This risk is highest in the first two years after you return to sport. This is due to underlying risk factors and compensation patterns.
An ACL injury unfortunately increases your long-term risk of developing osteoarthritis in that knee, regardless of whether you have surgery or not. However, surgery to restore stability significantly reduces this risk compared to leaving the knee unstable. An unstable knee that suffers from recurrent giving-way episodes and secondary meniscal tears will develop arthritis much faster.
If you are dealing with knee instability or think you may have torn your ACL, a specialist assessment is the right next step.
What to Bring: Please bring your referral letter, all relevant imaging studies (X-rays, CT scans, MRI if performed), and your list of current medications to your consultation.