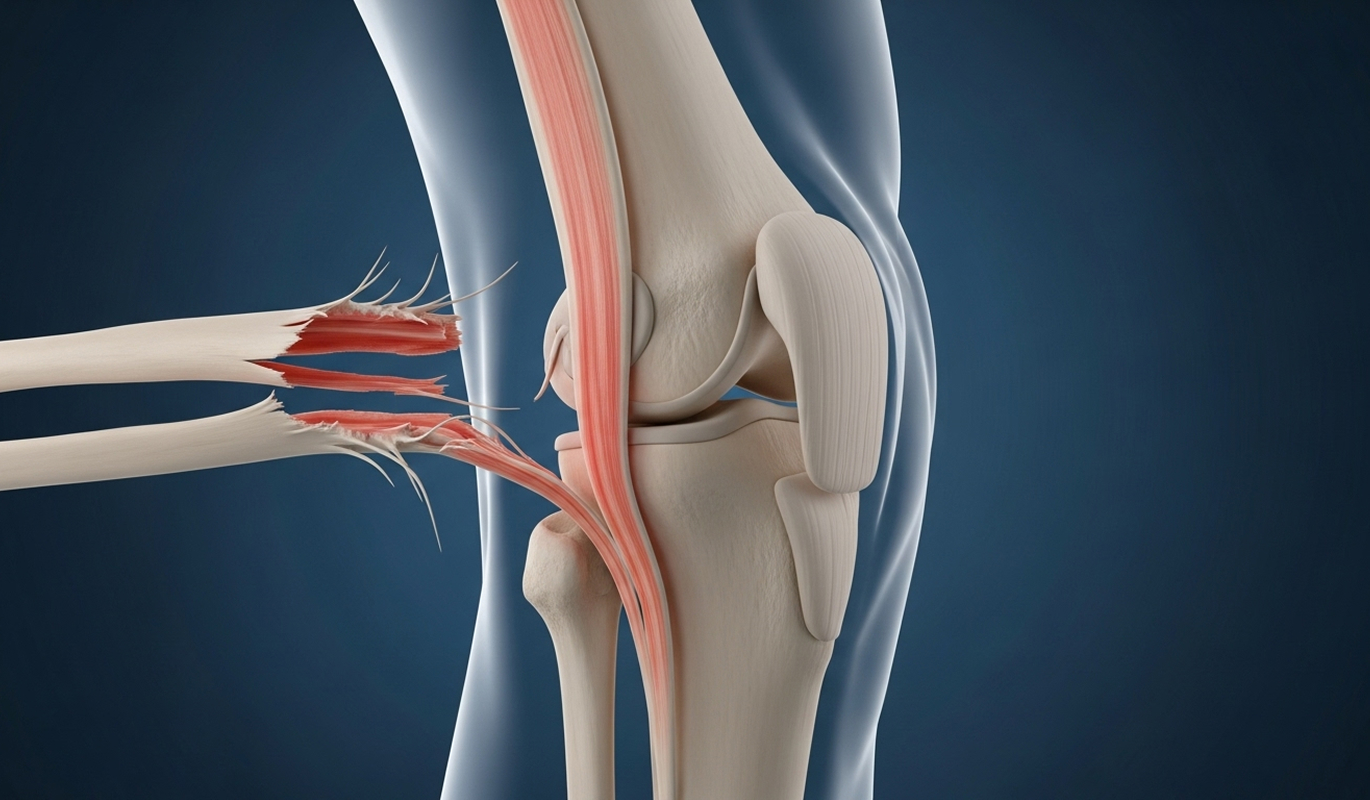
The ACL is vital for preventing excessive forward and rotational movement of the shinbone (tibia) relative to the thighbone (femur). This control is essential for sports involving cutting, pivoting, or sudden stops. A torn ACL leads to instability, where the knee can unexpectedly give way, increasing the risk of further damage to the meniscus or cartilage. Reconstruction aims to restore this crucial stability.
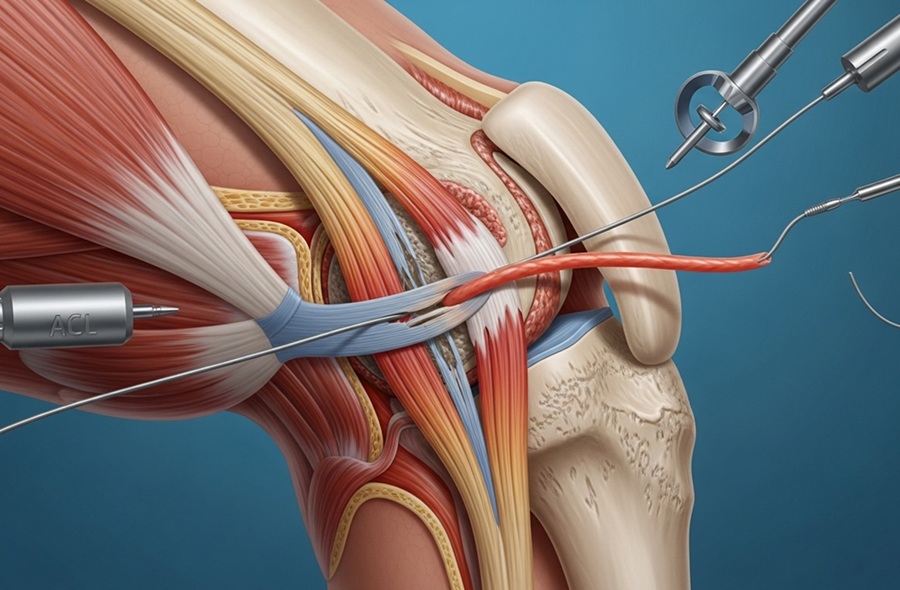
Dr Allom performs ACL reconstruction using arthroscopic (keyhole) techniques. This involves small incisions around the knee, through which a camera and specialised instruments are inserted. Compared to older open surgery methods, this approach typically results in less post-operative pain, smaller scars, and a faster initial recovery period. Most patients can go home the same day or after one night in hospital.
The primary goal for many patients undergoing ACL reconstruction is returning to sport or high-level activity. While outcomes vary, evidence shows that 80-90% of patients return to some level of sport, and 60-75% return to their pre-injury competitive level after surgery and comprehensive rehabilitation. Dr Allom follows strict, criteria-based guidelines to ensure a safe return to sport, typically around 9-12 months post-surgery.
Successful ACL reconstruction requires precise surgical technique. Dr Allom completed advanced fellowship training in sports knee surgery at prestigious UK institutions. He prefers using hamstring tendon autografts (your own tissue) for their strength and lower risk of donor site pain compared to other options, such as patellar tendon grafts, which can sometimes lead to anterior knee pain. The most critical step is creating bone tunnels in the exact anatomic footprint of the original ACL, ensuring the new graft functions correctly to restore both forward and rotational stability. This precision is key to long-term success.
Dr Allom considers your age, pre-injury activity level, future goals, occupation, and degree of instability when discussing treatment options.



Most athletes return to unrestricted sport between 9 and 12 months after surgery, once they meet all strength, functional, and psychological criteria. Returning earlier increases re-injury risk.
Yes, after a detailed discussion. Dr Allom typically recommends hamstring autograft due to its strength and lower donor site pain, but will consider other options (like patellar tendon) based on your specific situation and preferences.
This is common for many cases. Dr Allom prioritises repairing the meniscus whenever possible, which requires a stable knee provided by the ACL reconstruction. Meniscal repair may slightly extend your initial protected weight-bearing period.
Most patients (85-90%) achieve excellent function and high satisfaction, returning to demanding activities. However, the knee may feel subtly different. The goal is stable, pain-free function for your desired activities.
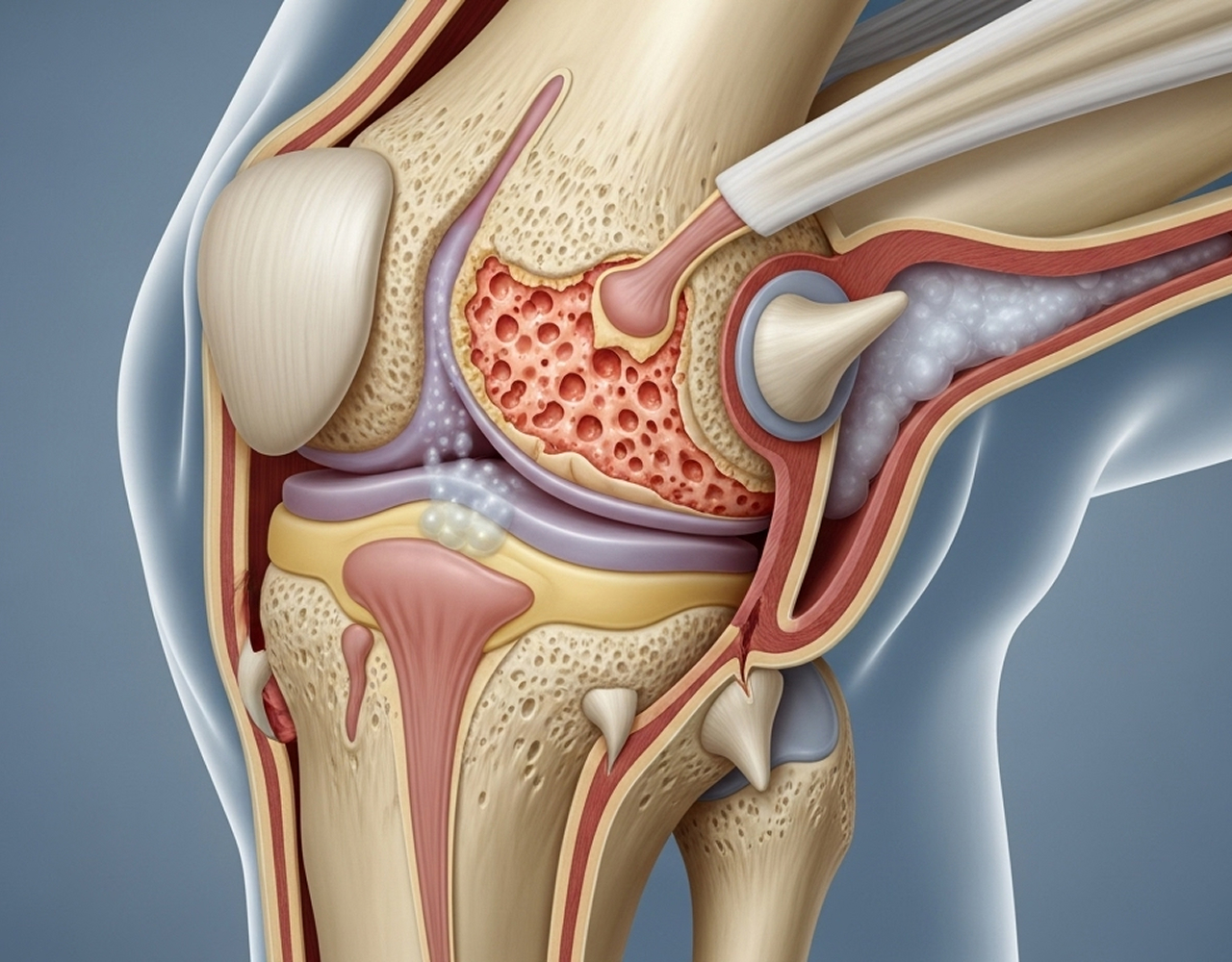
For active individuals, non-operative management often leads to ongoing instability, increased risk of further knee damage (meniscus, cartilage), and potentially earlier arthritis. It usually prevents a safe return to pivoting sports.
Yes. Age isn't the main factor. Activity level, goals, instability symptoms, and overall health are more important. Dr Allom treats many active patients in their 40s and 50s who wish to maintain demanding lifestyles.
If you have sustained an ACL injury or are experiencing knee instability, a specialist assessment with Dr Allom can determine the best treatment path for your goals.
What to Bring: Please bring your referral letter, all relevant imaging studies (X-rays, CT scans, MRI if performed), and your list of current medications to your consultation.